A Guide To The Modified Tardieu Scale
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, communicated or transmitted in any form or by any means without prior written permission by the copyright owner, except as permitted under the Australian Copyright Act 1968.
Epworth Rehabilitation has conducted a Spasticity Management Clinic at its campuses in Richmond and Hawthorn since 2009. In this specialised interdisciplinary clinic, patients with a wide variety of neurological diagnoses have their spasticity assessed and managed.
One of the key intentions of the clinic is to assess patient outcomes following treatment. The main outcomes involve changes in patient function and are measured by goal attainment scaling.
For measuring spasticity in individual muscles, we have adopted the use of the Modified Tardieu Scale. An issue with using this scale is in recording the measurements of each individual muscle with respect to starting positions, finishing positions and the angle at which a muscle response occurs.
Individual clinicians can use different techniques and angular measurements, which makes comparison of results before and after treatment inconsistent.
The aim of this App is to outline a protocol for the use of the Modified Tardieu Scale in the most commonly injected muscles of the upper and lower limb. This App has been compiled using the expertise of physiotherapists, occupational therapists and rehabilitation medicine physicians.
Acknowledgements
This App would not be possible without the generous support provided by the Epworth Medical Foundation, the Australian Physiotherapy Association and Physiotherapy ReSearch Epworth Rehabilitation (PRoSpER).
Contents
-
Upper Limb
-
Shoulder Rotators
- Pectoralis Major
- Subscapularis
- Teres Major
- Latissimus Dorsi
-
Elbow Flexors
- Biceps Brachii Long Head
- Brachialis
- Brachioradialis
-
Elbow Extensors
- Triceps Brachii Long Head
- Triceps Brachii Lateral Head
- Triceps Brachii Medial Head
-
Forearm Pronators
- Pronator Teres
- Pronator Quadratus
-
Wrist Flexors
- Flexor Carpi Radialis
- Flexor Carpi Ulnaris
-
Finger Flexors
- Flexor Digitorum Superficialis
- Flexor Digitorum Profundus
-
Thumb Muscles
- Flexor Pollicis Longus
- Flexor Pollicis Brevis
- Adductor Pollicis
-
Hand Muscles
- Intrinsic Finger Flexors (lumbricals)
-
Lower Limb
-
Hip Adductors
- Adductor Brevis
- Adductor Longus
- Adductor Magnus
-
Hip Flexors
- Psoas Major
-
Knee Flexors
- Semimembranosus
- Semitendinosus
- Biceps Femoris
-
Knee Extensors
- Vastus Lateralis
- Vastus Medialis
- Vastus Intermedius
- Rectus Femoris (prone)
- Rectus Femoris (supine)
-
Ankle Plantarflexors
- Gastrocnemius
- Soleus
-
Ankle Invertor
- Tibialis Posterior
-
Toe Flexors
- Flexor Digitorum Longus
- Flexor Digitorum Brevis
- Flexor Hallucis Longus
Glossary
- 10MWT 10 Metre Walk Test
- 6MWT 6 Minute Walk Test
- +ve Positive
- -ve Negative
- < Less than
- = Equals
- > Greater than
- AFO Ankle foot orthosis
- AL Adductor Longus
- AM Adductor Magnus
- APB Adductor Pollicis Brevis
- C1-7 Cervical spine level
- СТ Computed Tomography
- DF Dorsiflexion
- DIP Distal Interphalangeal
- FCR Flexor Carpi Radialis
- FCU Flexor Carpi Ulnaris
- FDL Flexor Digitorum Longus
- FDP Flexor Digitorum Profundus
- FDS Flexor Digitorum Superficialis
- FEM Femur
- FHL Flexor Hallucis Longus
- FPB Flexor Pollicis Brevis
- FPL Flexor Pollicis Longus
- Gastroc Gastrocnemius
- GHJ Glenohumeral Joint
- HUM Humerus
- IP Interphalangeal
- LUM Lumbricals
- L1-5 Lumbar spine level
- MCP Metacarpophalangeal
- PF Plantarflexion
- PG Plantargrade
- PIP Proximal Interphalangeal
- PQ Pronator Quadratus
- R Radius
- R1 The angle of muscle reaction
- R2 The angle of full range of motion
- REC FEM Rectus Femoris
- ROM Range of motion
- T1-12 Thoracic spine level
- TBI Traumatic Brain Injury
- Tib Tibia
- TS Tardieu Scale
- U Ulnar
- UN Ulnar Nerve
- US Ultrasound
- V1 Moving the limb as slow as possible
- V2 Moving the limb at the speed of the segment falling under gravity
- V3 Moving the limb as fast as possible
- X The dynamic tone component of the muscle
About the Tardieu Scale
The Tardieu Scale, which was originally developed by Guy Tardieu (Tardieu et al., 1954), is based on four key principles:
- Apply a passive stretch on a relaxed muscle.
- Maintain a consistent position of proximal segments.
- Measure the angle at which the resistance interrupts passive movement.
- Compare the angles of arrest in stretching manoeuvres of different speeds, from extremely slow to rapid (i.e., the spasticity angle).
Following multiple revisions by Held and Pierrot-Deseilligny (1969), Boyd and Graham (1999) and Gracies et al. (2010), the Tardieu Scale evolved to the version known presently as the Modified Tardieu Scale.
Both the Tardieu Scale and the Modified Tardieu Scale involve testing the resistance of spastic muscles to passive stretching at different velocities and grading the resistance, using an ordinal scale.
The Starting Position
Standardise the resting positions prior to stretching the muscle.
Based on the definition of R2 being the full ROM of the joint, the starting position of the muscle being tested should be at rest in its shortest position.
The more distal joint is held in the shortest position (for multi-joint muscles) whereas the proximal joint is held in a standardised position, throughout.
For example, when measuring finger flexors, the wrist is held at 30° extension to start the stretch, not at maximum flexion.
The angle, zero, is based on the anatomical position.
Use a quiet room with minimal stimulation and, if possible, at the same time of day as the previous assessment.
Other body segments, particularly head and neck, should also be maintained in a standardised position.
Test the upper limb in the sitting position.
The elbow should be flexed to 90° and the shoulder held in a neutral position when testing the wrist and fingers.
Test the lower limb in a supine position.
Limit and keep the number of stretching manoeuvres consistent prior to the V1/V3 test, as they will impact on stretch reflex excitability.
Modifications to the starting position
Where contracture or pain limit the ability to attain the designated starting position for a muscle, reduce the starting position of the proximal joint and document for repeatability.
Then the patient is unable to attain the suggested testing position, i.e. they are unable to lie prone, modify the testing position to ensure patient comfort with the muscle relaxed
For muscles not included in this guide, apply the principles of Modified Tardieu Scale testing outlined above.
Modified Tardieu Scale Criteria
The most recent versions of the scale use the following criteria:
Patients are positioned sitting to test the upper limbs and supine to test the lower limbs.
Four measurements:
- The angle of ROM during V1 (R2)
- The angle of muscle reaction during V3 (R1)
- The quality of muscle reaction during V3 (0-5)
- The dynamic tone component of the muscle (X)
Three speed definitions:
- V1 is moving the limb as slow as possible
- V2 is moving the limb at the speed of the segment falling under gravity
- V3 is moving the limb as fast as possible
Quality of Muscle Reaction score (0-5):
- 0 is no resistance to passive ROM
- 1 is slight resistance during passive movement with no clear catch
- 2 is a clear catch at a precise angle followed by a release
- 3 is fatiguable clonus (< 10 seconds when maintaining the pressure)
- 4 is unfatiguable clonus (> 10 seconds when maintaining the pressure)
- 5 is an immovable joint
The angle of full ROM (R2) is taken at a very slow speed (V1) measured with a universal goniometer. The angle of muscle reaction (R1) is defined as the angle at which a catch or clonus is found during a quick stretch (V3), and is measured with the goniometer.
The difference between R2 and R1 is referred to as the spasticity angle and reflects the dynamic tone component of the muscle. The larger the spasticity angle, the more spastic the muscle.
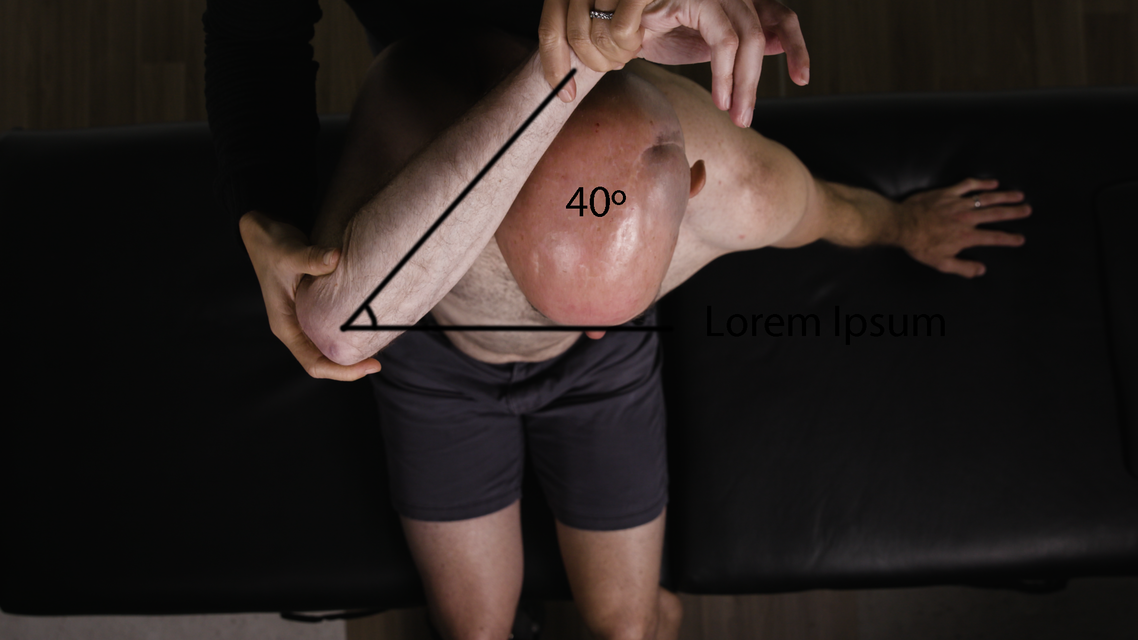
Pectoralis Major
Shoulder Rotators
| Pectoralis Major | |
|---|---|
| Action | Internal rotation of the shoulder joint, adduction of the arm. |
| Origin | Medial half of the clavicle and anterior surfaces of the sternum and cartilages of the first six ribs. |
| Insertion | Lateral lip of the bicipital groove of the humerus. |
| Innervation | Medial Pectoral Nerve (C7, C8, T1) and lateral pectoral nerve (C5, C6). |
| Tardieu Testing | |
| Patient position | Sitting. |
| Measurement considerations | Neutral GHJ rotation = 0° External rotation = +ve Internal rotation = -ve |
| Starting limb position | Shoulder abducted to 90°, GHJ maximum internal rotation. Elbow flexed at 90°, forearm neutral. |
| End limb position | Maximum external rotation of GHJ, with shoulder maintaining the same abduction angle. |
| Other considerations | Patient may lie supine, especially if the shoulder is painful, otherwise, a second person is required to stabilise the scapula and the GHJ in the sitting position. The sternocostal head of the muscle, which is the larger part, is the prime mover for horizontal flexion. The clavicular head assists in shoulder flexion, while the sternocostal head assists with shoulder extension from a flexed position. |
Goniometer landmarks

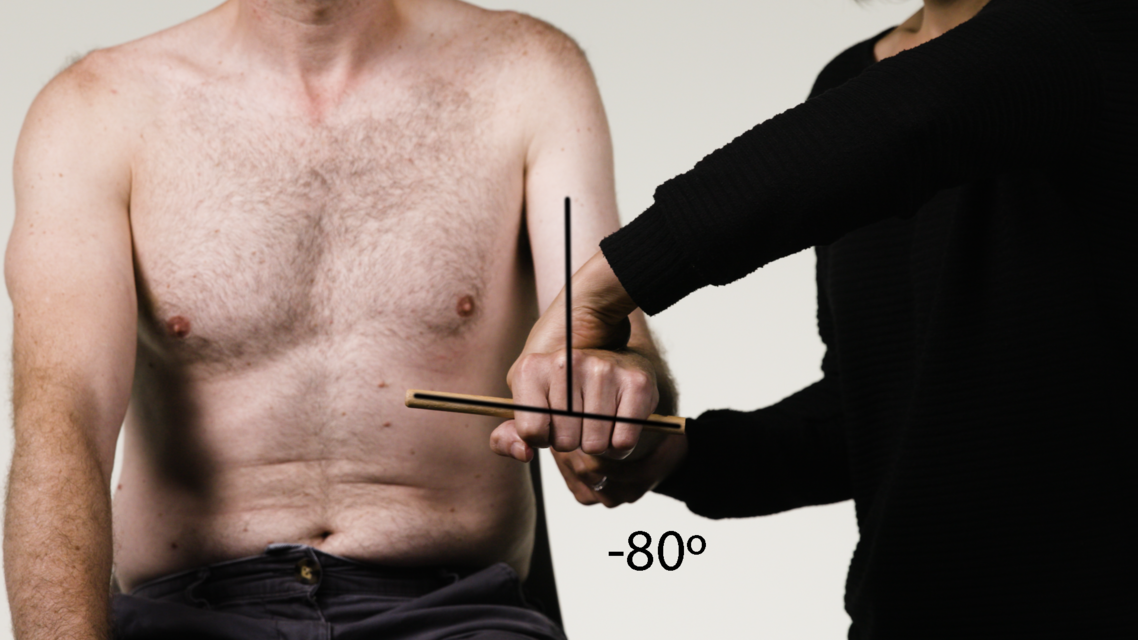
START:Control
Starting position: -40° external rotationStationary arm: horizontal
Axis: elbow joint
Moving arm: forearm
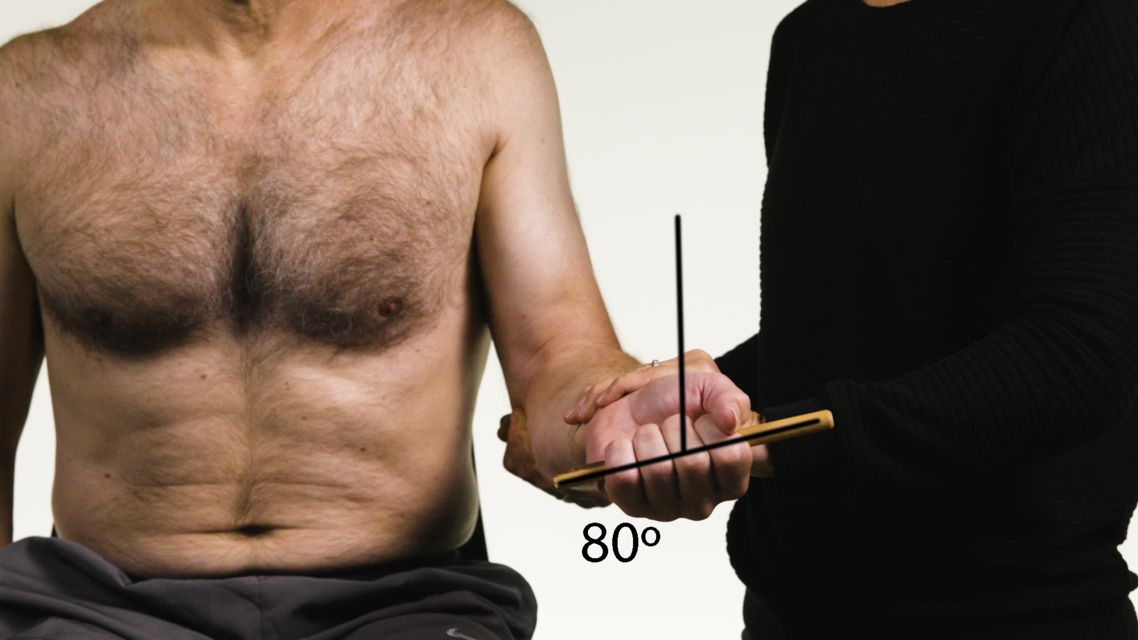
FINISH:Control
Finishing position(R2): 80° external rotationStationary arm: horizontal
Axis: elbow joint
Moving arm: forearm
Control - Coronal (front) view
Control - Lateral view
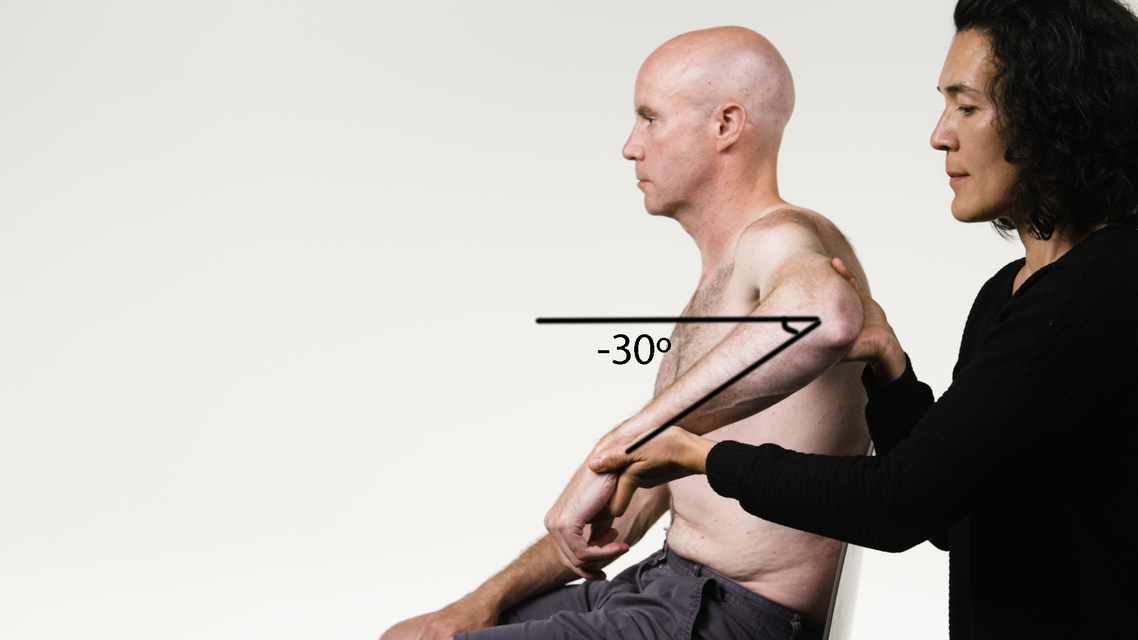
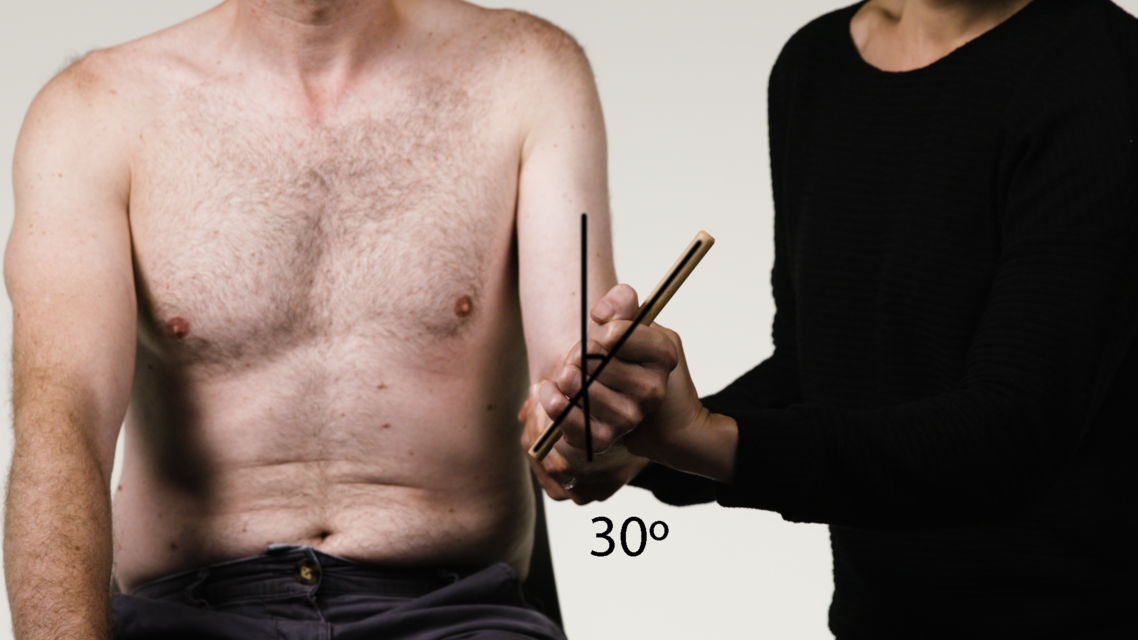
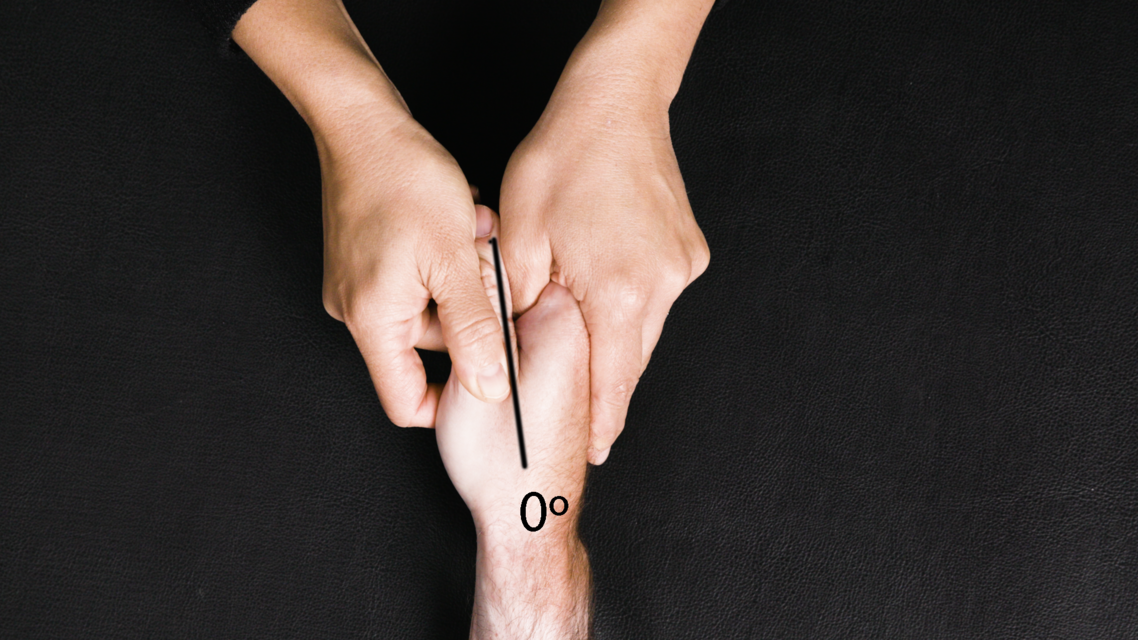
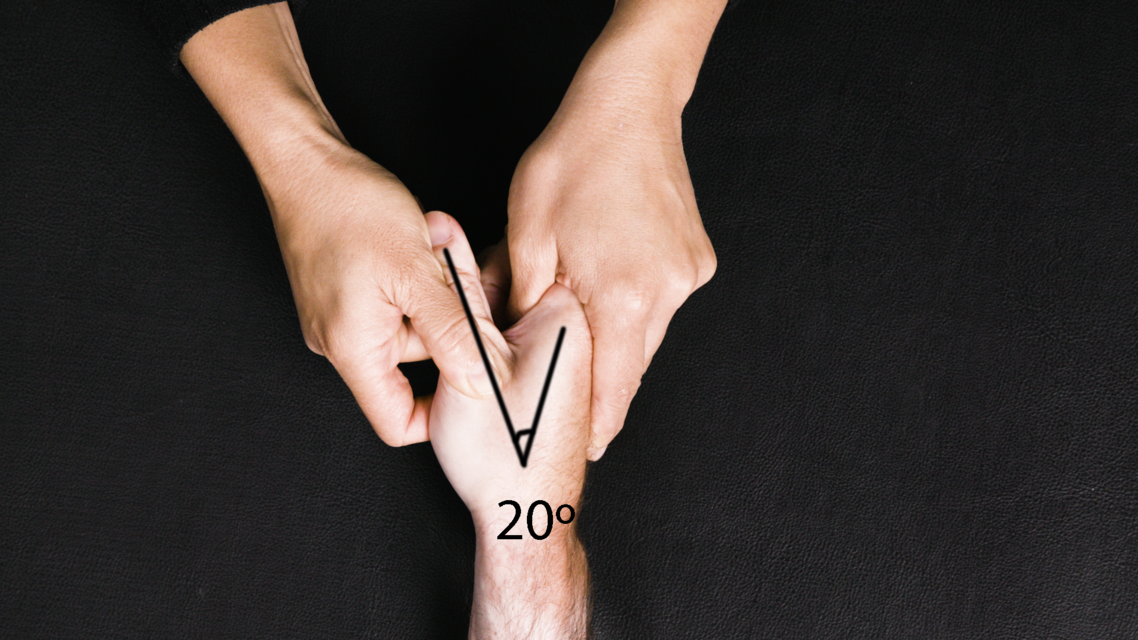
START:Patient
Starting position: -30° external rotationStationary arm: horizontal
Axis: elbow joint
Moving arm: forearm

FINISH:Patient
Finishing position(R2): 20° external rotationStationary arm: horizontal
Axis: elbow joint
Moving arm: forearm

REACTION:Patient
Angle of muscle reaction (R1): 0° external rotationStationary arm: horizontal
Axis: elbow joint
Moving arm: forearm
Spasticity angle = 20°
Patient - Coronal (front) view
Patient - Lateral view
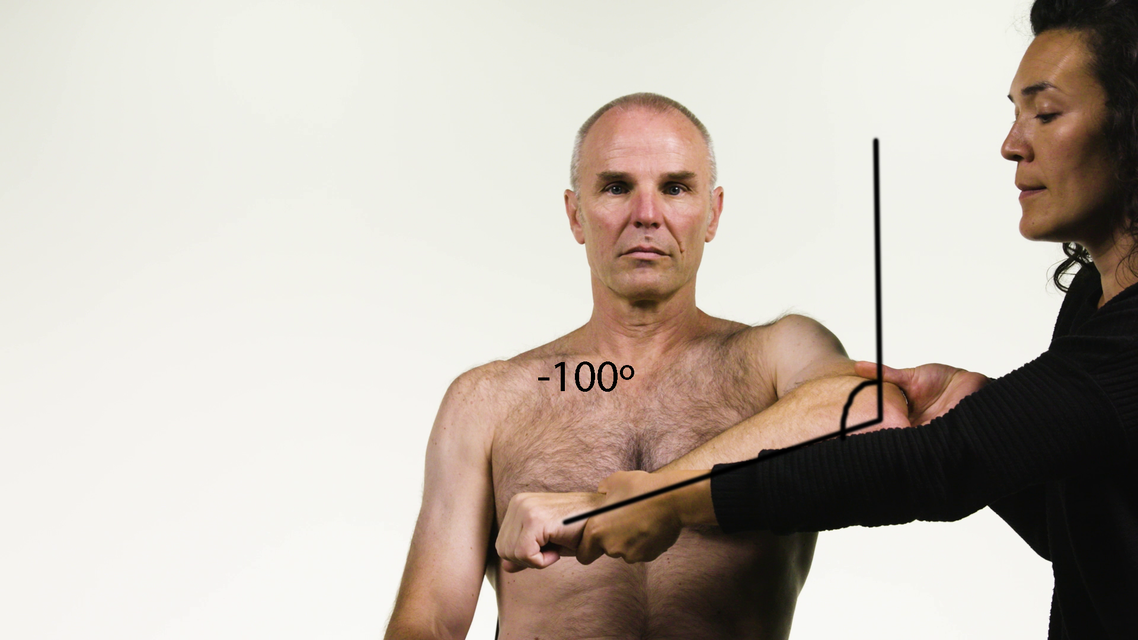
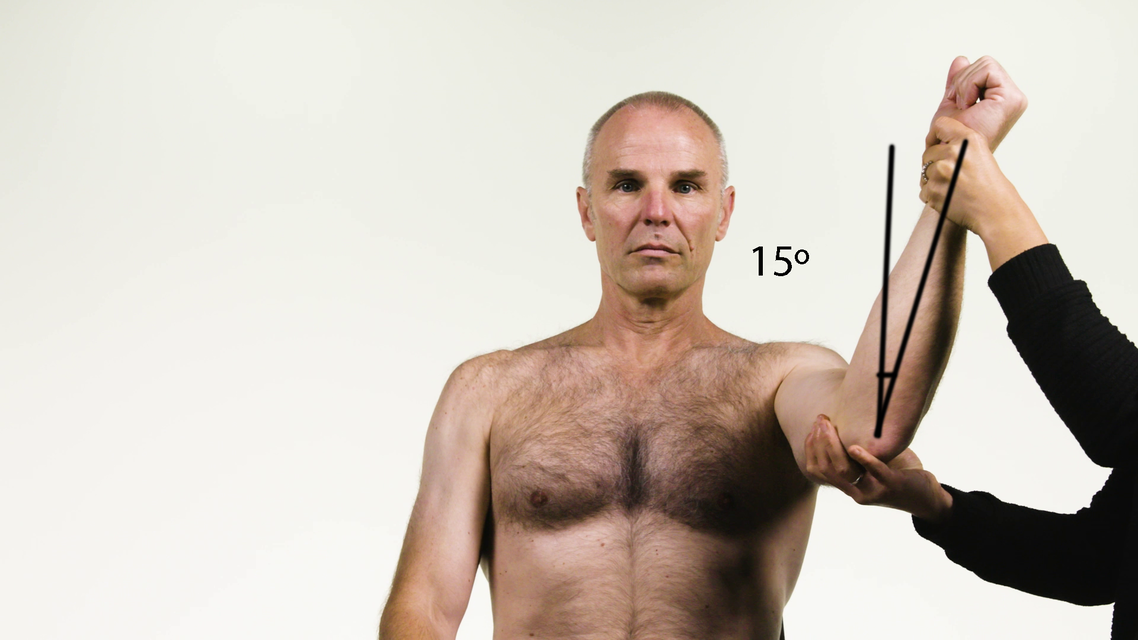
Subscapularis
Shoulder Rotators
| Subscapularis | |
|---|---|
| Action | Internal rotation and adduction of the humerus, stabilisation of the shoulder. |
| Origin | Subscapular fossa. |
| Insertion | Lesser tubercle of the humerus. |
| Innervation | Upper subscapular nerve, lower subscapular nerve (C5, C6). |
| Notes | Latissimus dorsi is a much stronger adductor than subscapularis and, therefore, subscapularis is tested in flexion to minimise the impact of latissimus dorsi on testing. It is most important that the clinician palpate and observe the muscles around the shoulder. |
| Tardieu Testing | |
| Patient position | Sitting. |
| Measurement considerations | Neutral GHJ rotation = 0° Internal rotation = -ve External rotation = +ve |
| Starting limb position | Shoulder flexed to 90°, elbow flexed to 90°. Maximum internal rotation of the GHJ. |
| End limb position | Maximum external rotation of the GHJ. |
| Other considerations | Subscapularis is under the scapula and can be accessed laterally. Palpate to differentiate between teres major. Patient may lie supine, especially if the shoulder is painful, otherwise a second person to stabilise the scapula and GHJ in the sitting position is required. When the arm is raised, subscapularis draws the humerus forward and downward. |
Goniometer landmarks
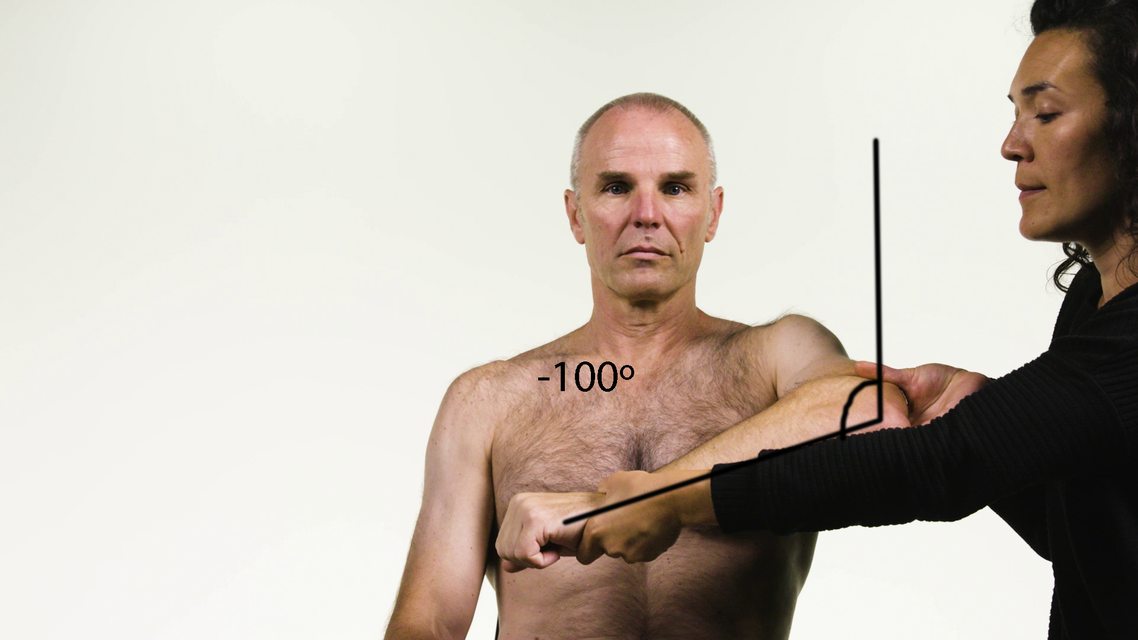
START:Control
Starting position: -100° external rotationStationary arm: vertical
Axis: elbow joint
Moving arm: forearm
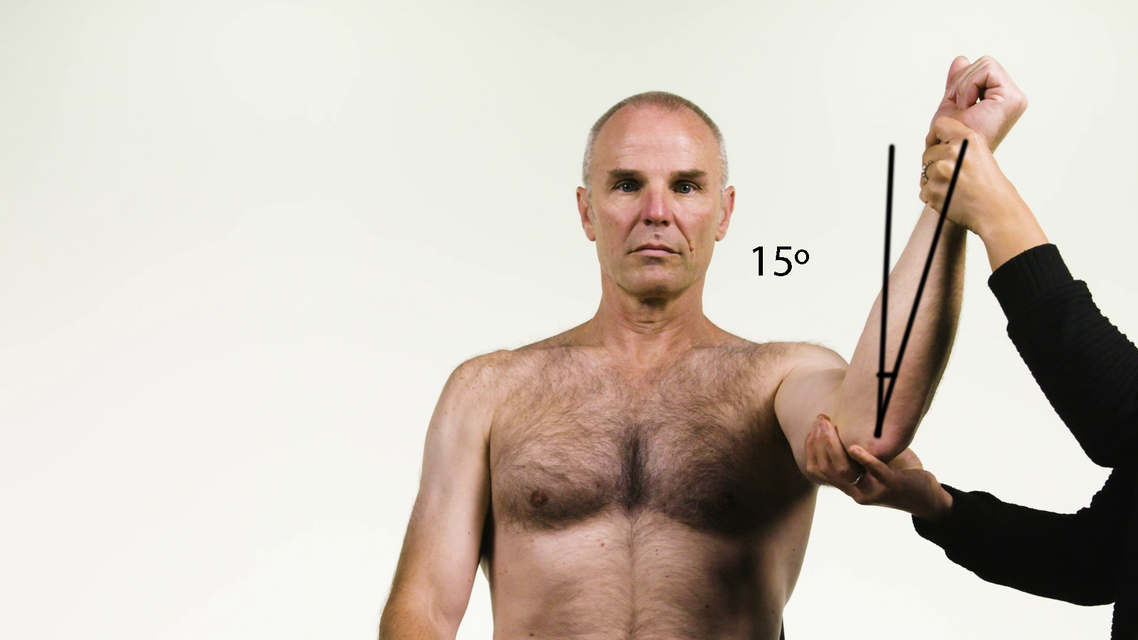
FINISH:Control
Finishing position(R2): 15° external rotationStationary arm: vertical
Axis: elbow joint
Moving arm: forearm
Control - Coronal (front) view

START:Patient
Starting position: -90° external rotationStationary arm: vertical
Axis: elbow joint
Moving arm: forearm

FINISH:Patient
Finishing position(R2): 5° external rotationStationary arm: vertical
Axis: elbow joint
Moving arm: forearm

REACTION:Patient
Angle of muscle reaction (R1): -5° external rotationStationary arm: vertical
Axis: elbow joint
Moving arm: forearm
Spasticity angle = 10°
Patient - Coronal (front) view
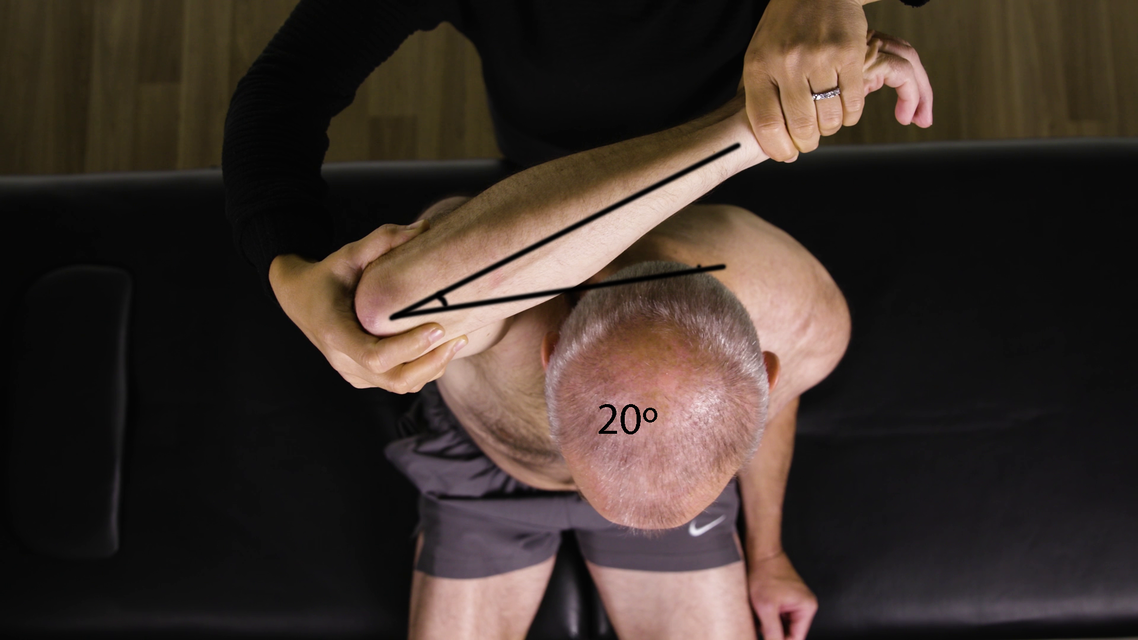
Teres Major
Shoulder Rotators
| Teres Major | |
|---|---|
| Action | Internal rotation of the shoulder joint. |
| Origin | Inferior angle of the scapular. |
| Insertion | Medial ridge of the bicipital groove of the humerus. |
| Innervation | Lower subscapular nerve (C5, C6). |
| Notes | Latissimus dorsi is a much stronger adductor than teres major and, therefore, testing of teres major is performed in flexion to minimise the impact of latissimus dorsi. Teres major is an internal rotator and adductor of the humerus and assists latissimus dorsi in drawing the previously raised humerus downwards and backwards. It also helps to stabilise the humeral head in the glenoid cavity. It is most important that the clinician palpate and observes the muscles around the shoulder. |
| Tardieu Testing | |
| Patient position | Sitting. |
| Measurement considerations | Neutral GHJ rotation = 0° Internal rotation = -ve External rotation = +ve |
| Starting limb position | Shoulder flexed to 90°, elbow flexed to 90°. Maximum internal rotation of the GHJ. |
| End limb position | Maximum external rotation of the GHJ. |
| Other considerations | Palpate to differentiate between subscapularis. Teres major is more superficial. The patient may lie supine, especially if the shoulder is painful, otherwise, a second person to stabilise the scapula and GHJ in the sitting position is required. |
Goniometer landmarks
START:Control
Starting position: -100° external rotationStationary arm: vertical
Axis: elbow joint
Moving arm: forearm
FINISH:Control
Finishing position(R2): 15° external rotationStationary arm: vertical
Axis: elbow joint
Moving arm: forearm
Control - Coronal (front) view

START:Patient
Starting position: -90° external rotationStationary arm: vertical
Axis: elbow joint
Moving arm: forearm

FINISH:Patient
Finishing position(R2): 5° external rotationStationary arm: vertical
Axis: elbow joint
Moving arm: forearm

REACTION:Patient
Angle of muscle reaction (R1): -5° external rotationStationary arm: vertical
Axis: elbow joint
Moving arm: forearm
Spasticity angle = 10°
Patient - Coronal (front) view
Latissimus Dorsi
Shoulder Rotators
| Latissimus Dorsi | |
|---|---|
| Action | Internal rotation, adduction and extension of the arm. |
| Origin | Spinous processes of the lower thoracic vertebrae, lumbosacral fascia and posterior crest of the ilium. |
| Insertion | Intertubercular groove of the humerus. |
| Innervation | Thoracodorsal nerve (C6, C7, C8). |
| Tardieu Testing | |
| Patient position | Sitting, with a second person to stabilise the scapula and GHJ. Laterally flex the patient’s trunk away from the arm being measured. The patient may lie supine, especially if the shoulder is painful. |
| Measurement considerations | Neutral GHJ rotation = 0° Internal rotation = -ve External rotation = +ve |
| Starting limb position | Shoulder in maximum abduction. Maximum internal rotation of the GHJ. |
| End limb position | Maximum external rotation of the GHJ. |
| Other considerations | Palpate to differentiate between teres, subscapularis and pectoralis. Many patients will have difficulty achieving this range of abduction, so document abduction angle that test is completed in. |
Goniometer landmarks

START:Control
Starting position: -25° external rotationStationary arm: transverse plane
Axis: elbow joint
Moving arm: forearm
FINISH:Control
Finishing position(R2): 20° external rotationStationary arm: transverse plane
Axis: elbow joint
Moving arm: forearm
Control - Coronal (front) view
Control - Aerial view

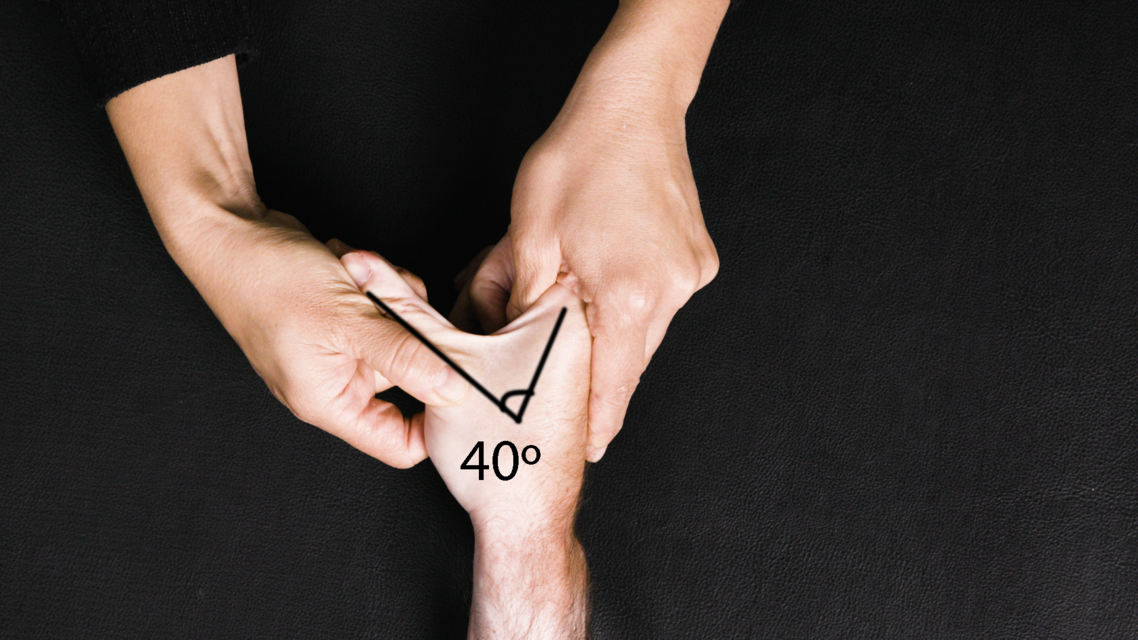
START:Patient
Starting position: -20° external rotationStationary arm: transverse plane
Axis: elbow joint
Moving arm: forearm
FINISH:Patient
Finishing position(R2): 40° external rotationStationary arm: transverse plane
Axis: elbow joint
Moving arm: forearm

REACTION:Patient
Angle of muscle reaction (R1): 15° external rotationStationary arm: transverse plane
Axis: elbow joint
Moving arm: forearm
Spasticity angle = 25°
Patient - Coronal (front) view
Patient - Aerial view
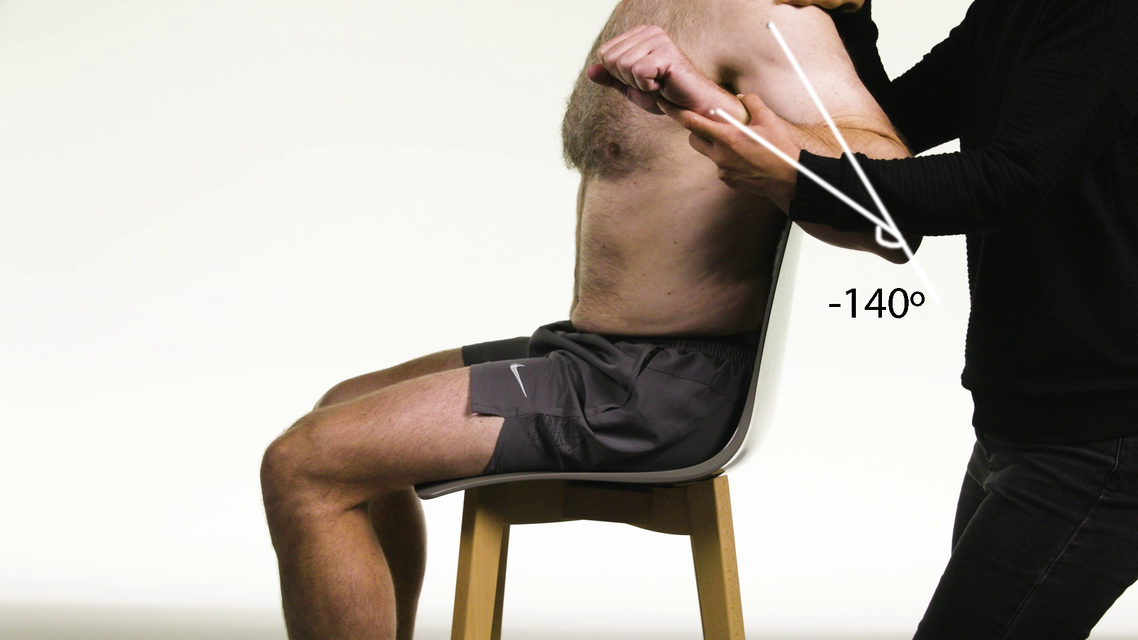
Biceps Brachii Long Head
Elbow Flexors
| Biceps Brachii Long Head | |
|---|---|
| Action | Supination and flexion at the elbow. |
| Origin | Long head: supraglenoid tubercle of scapula. |
| Insertion | Radial tuberosity. |
| Innervation | Musculocutaneous nerve (C5, C6). |
| Notes | The long head of the biceps helps to flex the shoulder in the first 30° of elevation. The short (distal/anterior) and long heads have distinct insertions. The short head insertion allows greater efficiency of elbow flexion at 90°. The short head is a more efficient supinator when the forearm is in pronation or neutral. The long head is a more efficient supinator when the forearm is in supination. The long head assists in shoulder flexion. In general, the biceps brachii is the primary and most powerful supinator of the forearm and supinates the forearm in the absence of resistance. |
| Tardieu Testing | |
| Patient position | Sitting with the scapula and head of the humerus supported. |
| Measurement considerations | Maintain maximum forearm pronation throughout test. Elbow in full extension = 0° Flexion = -ve |
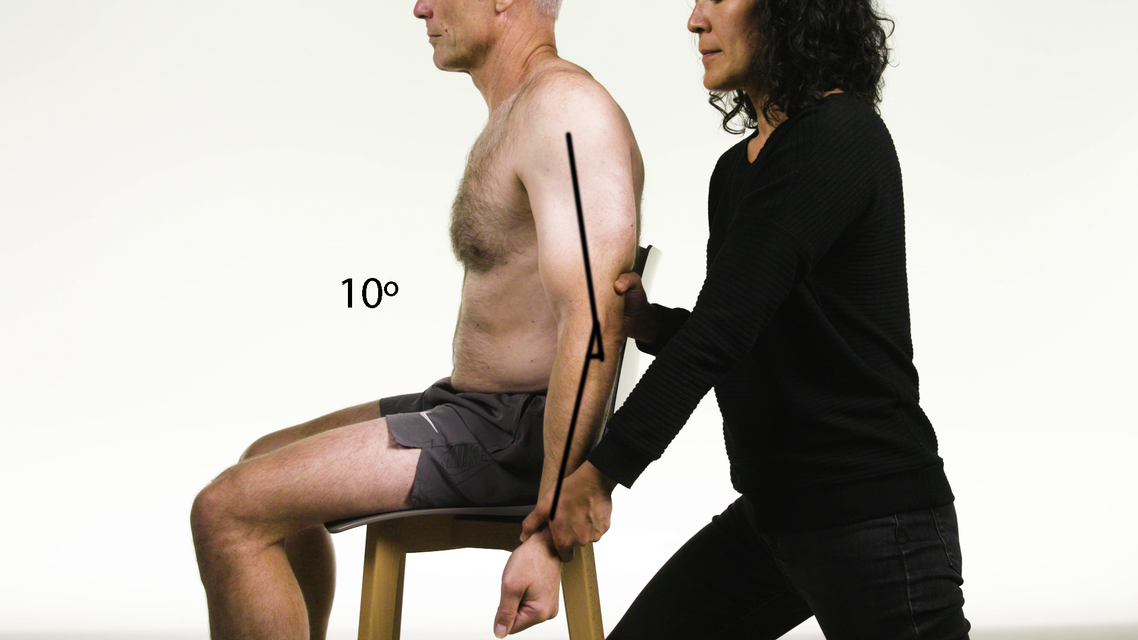
| Starting limb position | The shoulder is placed in 10° of extension. Maximum elbow flexion, maximum forearm pronation. |
| End limb position | Maximum elbow extension. |
| Other considerations | It is technically not possible to differentiate the elbow flexors through the forearm position. The protocol is based on the position that will most likely place the muscle in maximum stretch. Palpation and observation are integral to differentiation. When determining whether to inject this muscle, the clinician must consider the role of the biceps brachii as an active supinator. The clinician must consider not injecting the biceps brachii if pronation is the primary resting position and the pronators are also spastic. |
Goniometer landmarks
START:Control
Starting position: -140° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm

FINISH:Control
Finishing position(R2): 0° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
Control - Lateral view

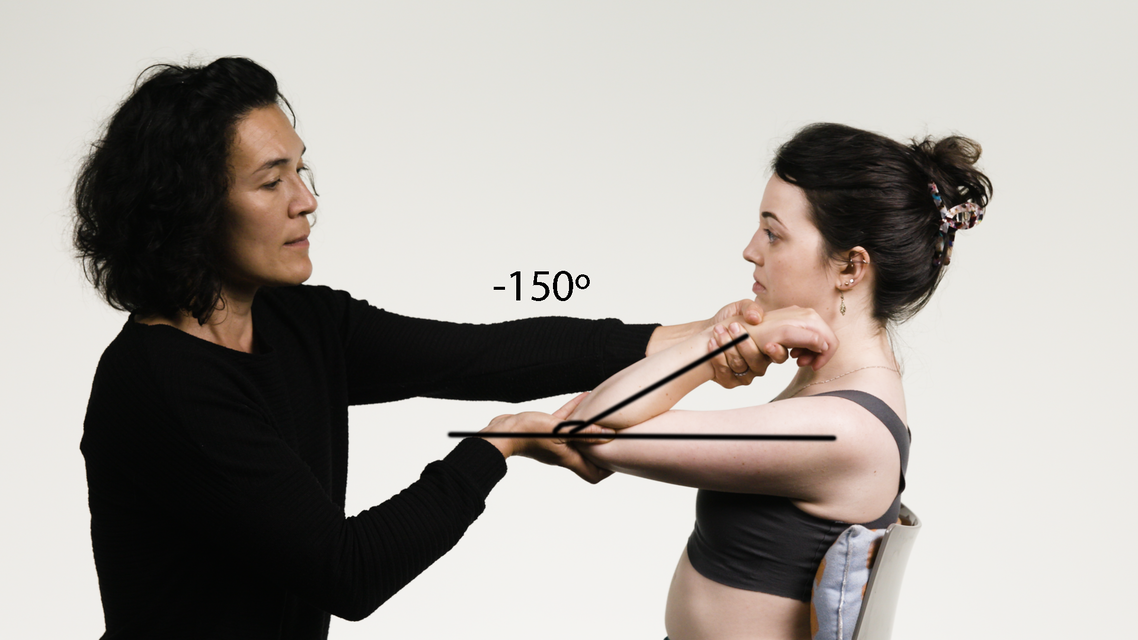
START:Patient
Starting position: -150° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm

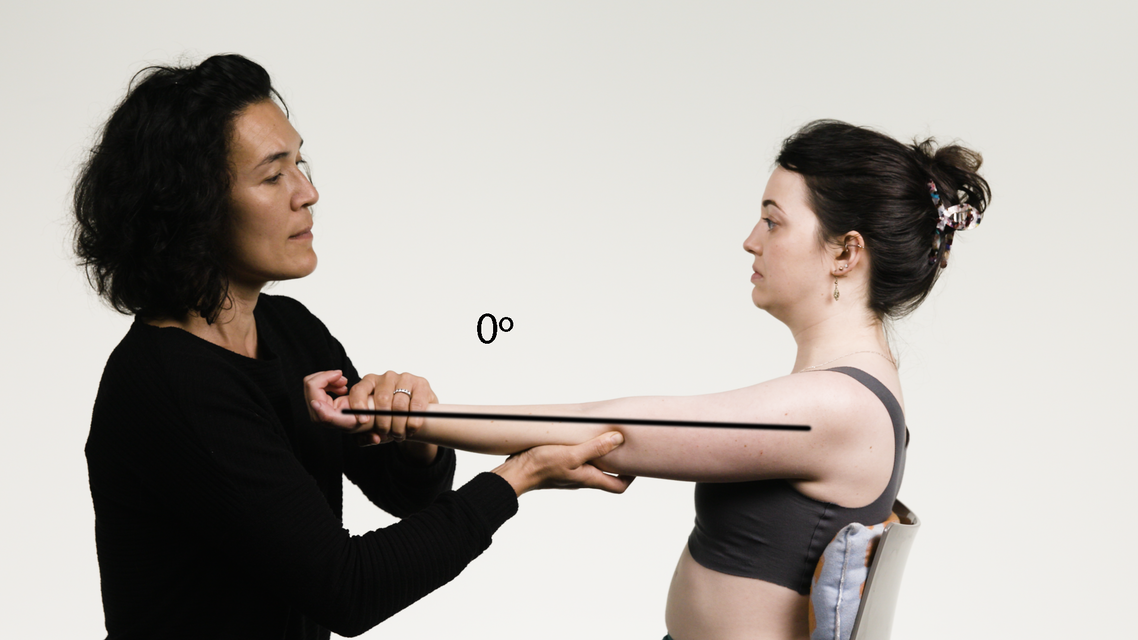
FINISH:Patient
Finishing position(R2): -10° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm

REACTION:Patient
Angle of muscle reaction (R1): -60° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
Spasticity angle = 50°
Patient - Lateral view
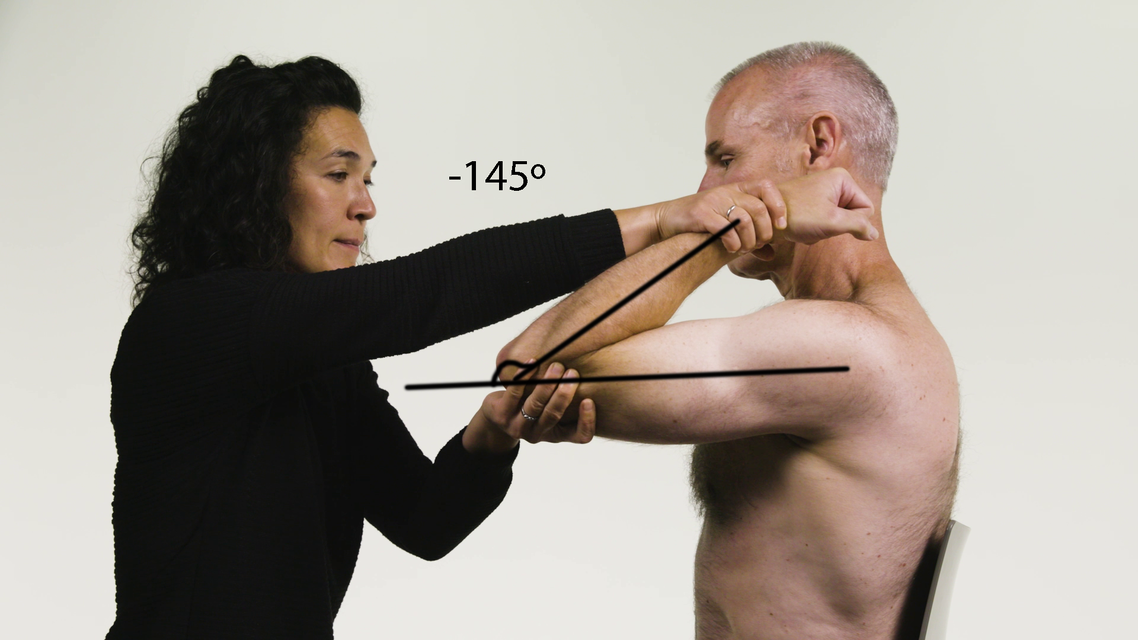
Brachialis
Elbow Flexors
| Brachialis | |
|---|---|
| Action | Flexion at elbow. |
| Origin | Anterior surface of the distal half of the humerus and medial intermuscular septum. |
| Insertion | Ulnar tuberosity and volar surface of the coronoid process. |
| Innervation | Musculocutaneous nerve (C5, C6). |
| Notes | The brachialis is the strongest flexor of the elbow joint, as it is closer to the axis of the joint and only stretches over one joint in contrast to the biceps. A small contraction of the muscle consequently leads to a larger flexion of the elbow. It makes up the floor of the cubital fossa. |
| Tardieu Testing | |
| Patient position | Sitting, with the scapula and head of the humerus supported. |
| Measurement considerations | Elbow in full extension = 0° Flexion = -ve |
| Starting limb position | Shoulder flexion to 90° Neutral GHJ rotation = 0° Maximum forearm supination and maximum elbow flexion. |
| End limb position | Maintain shoulder and GHJ position, as above and maximum elbow extension and forearm supination. |
| Other considerations | It is technically not possible to differentiate the elbow flexors through the forearm position. The protocol is based on the position that will most likely place the muscle in maximum stretch. Palpation and observation are integral to differentiation. If unable to supinate the forearm, the clinician should simply test brachialis in a comfortable forearm position. If unable to flex the shoulder to 90°, test brachialis in a comfortable shoulder flexion, to take the stretch off the long head of biceps brachii. |
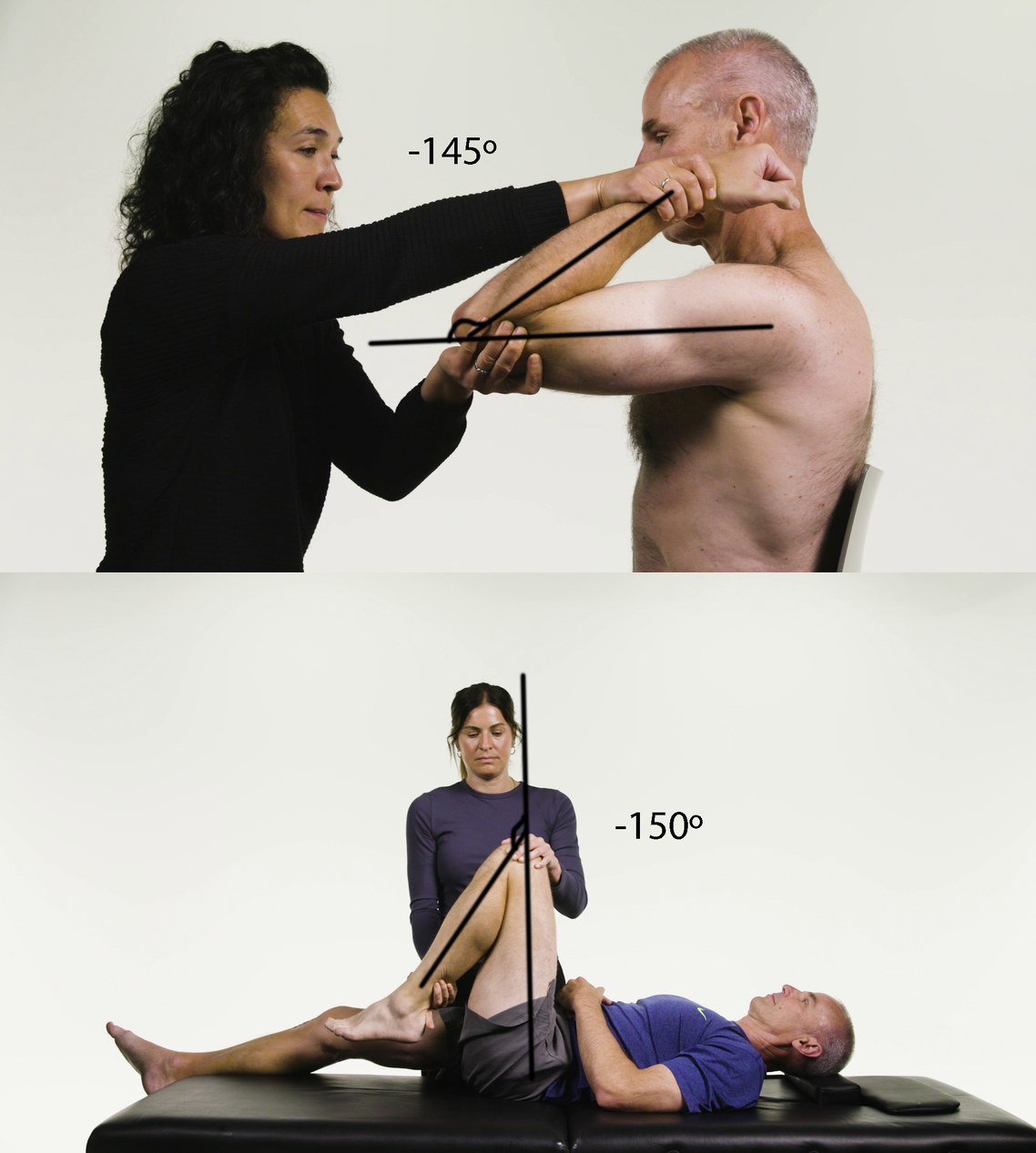
Goniometer landmarks
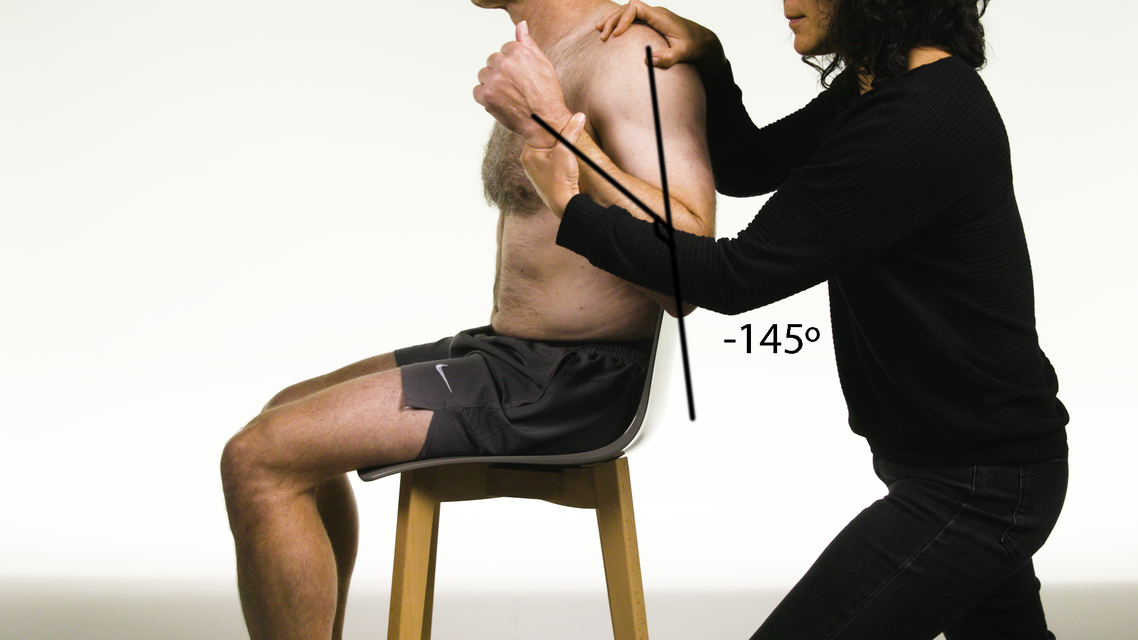
START:Control
Starting position: -145° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
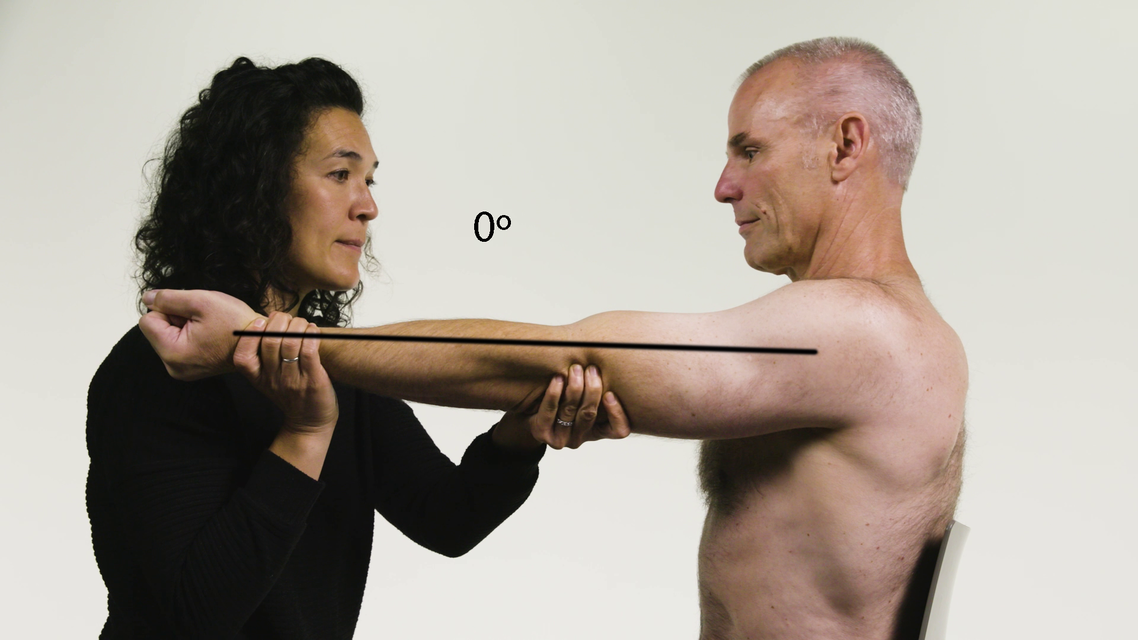
FINISH:Control
Finishing position(R2): 0° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
Control - Lateral view
START:Patient
Starting position: -150° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
FINISH:Patient
Finishing position(R2): 0° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm

REACTION:Patient
Angle of muscle reaction (R1): -30° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
Spasticity angle = 30°
Patient - Lateral view
Brachioradialis
Elbow Flexors
| Brachioradialis | |
|---|---|
| Action | Flexion at elbow with the forearm in mid-prone position. |
| Origin | Lateral supracondylar ridge of the humerus. |
| Insertion | Base of the radial styloid. |
| Innervation | Radial nerve (C5, C6). |
| Notes | Brachioradialis is capable of both pronation and supination, depending on the position of the forearm. |
| Tardieu Testing | |
| Patient position | Sitting, with the scapula and head of the humerus supported. |
| Measurement considerations | Maintain mid-prone forearm position throughout the test. Maximum elbow extension = 0° Flexion = -ve |
| Starting limb position | GHJ neutral. Maximum elbow flexion in mid-prone forearm position. |
| End limb position | Maximum elbow extension, while maintaining mid-prone forearm position. |
| Other considerations | It is technically not possible to differentiate the elbow flexors through the forearm position. The protocol is based on the position that will most likely place the muscle in maximum stretch. Palpation and observation are integral to differentiation. If unable to achieve a neutral forearm position, palpate to differentiate between the biceps brachii and brachialis. |
Goniometer landmarks
START:Control
Starting position: -145° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm

FINISH:Control
Finishing position(R2): 0° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
Control - Lateral view

START:Patient
Starting position: -155° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm

FINISH:Patient
Finishing position(R2): -10° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
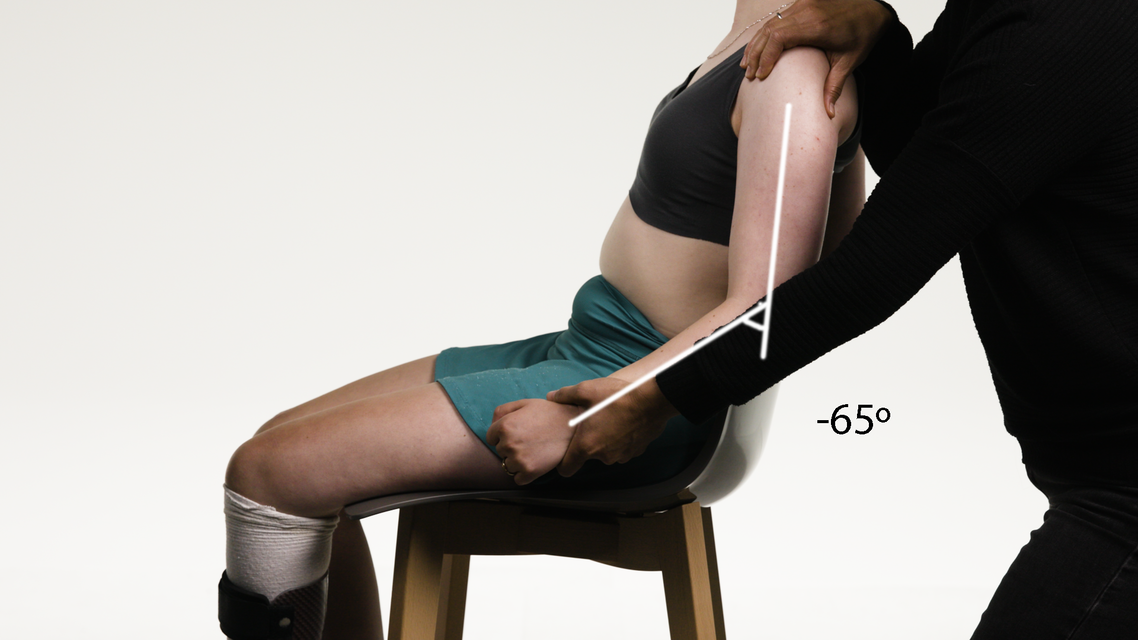
REACTION:Patient
Angle of muscle reaction (R1): -65° extensionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
Spasticity angle = 55°
Patient - Lateral view
Triceps Brachii Long Head
Elbow Extensors
| Triceps Brachii Long Head | |
|---|---|
| Action | Extension at elbow, extension at shoulder (long head). |
| Origin | Infraglenoid tubercle of the scapula. |
| Insertion | Via a common tendon, the three heads of triceps brachii insert into the dorsal aspect of the olecranon of the ulna. |
| Innervation | Radial nerve (C7, C8, T1). |
| Tardieu Testing | |
| Patient position | Sitting, with the scapula and head of the humerus supported. |
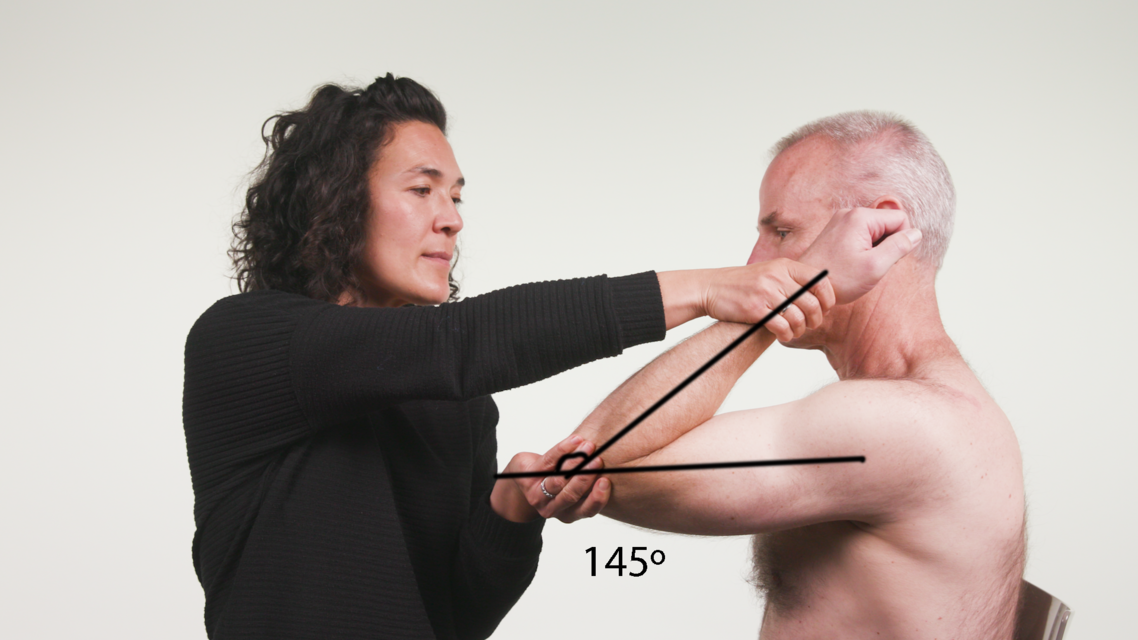
| Measurement considerations | Maximum elbow flexion = approximately 145 ̊ Full extension = 0 ̊ Flexion = +ve |
| Starting limb position | Shoulder flexed to 90 ̊, maximum elbow extension, forearm supination. |
| End limb position | Maximum elbow flexion, forearm supination. To differentiate between the long, lateral and medial heads of the triceps brachii, bring the GHJ into 90 ̊ of flexion. Palpate to differentiate between the three heads of triceps brachii. |
| Other considerations | Each head of the triceps brachii has a different pattern of force and activity during different shoulder elevations. The long head contributes to elbow extension more at shoulder elevation and the medial head takes over at > 90° of shoulder elevation. |
Goniometer landmarks

START:Control
Starting position: 0° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
FINISH:Control
Finishing position(R2): 145° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
Control - Lateral view

START:Patient
Starting position: 15° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
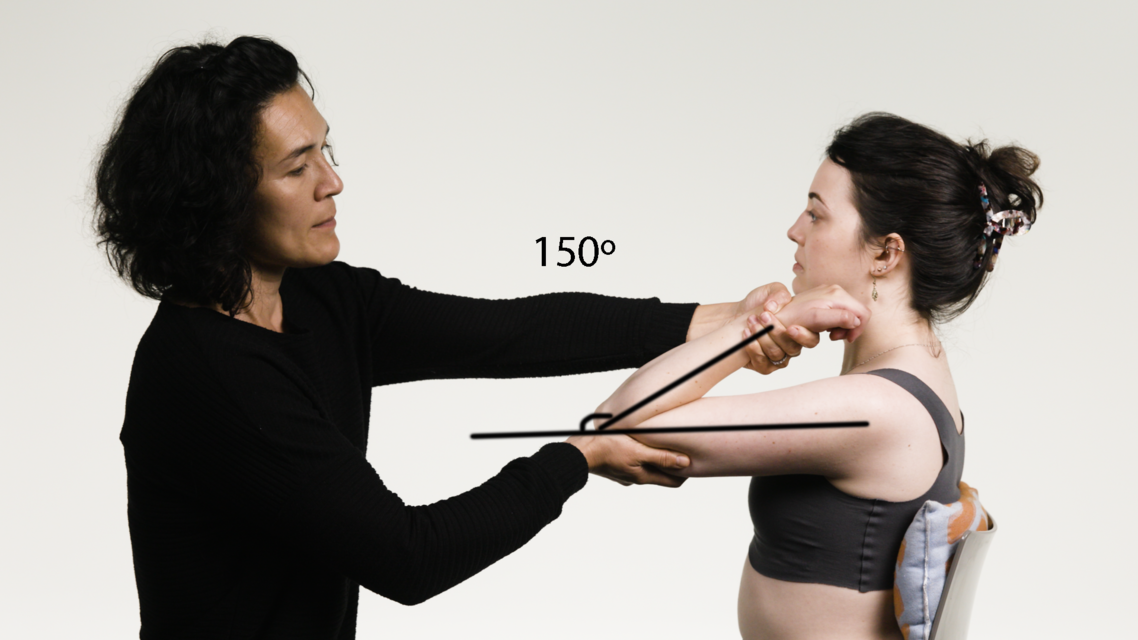
FINISH:Patient
Finishing position(R2): 150° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm

REACTION:Patient
Angle of muscle reaction (R1): 95° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
Spasticity angle = 55°
Patient - Lateral view
Triceps Brachii Lateral Head
Elbow Extensors
| Triceps Brachii Lateral Head | |
|---|---|
| Action | Extension at elbow. |
| Origin | Dorsal surface of the humerus above the groove for the radial nerve. |
| Insertion | Via a common tendon, the three heads of triceps brachii insert into the dorsal aspect of the olecranon of the ulnar. |
| Innervation | Radial nerve (C7, C8, T1). |
| Injection site | Immediately posterior to the insertion of deltoid. |
| Notes | There is choice regarding which head of triceps to inject. |
| Tardieu Testing | |
| Patient position | Sitting, with the scapula and head of the humerus supported. |
| Measurement considerations | Maximum elbow flexion = approximately 145 ̊ Full extension = 0 ̊ Flexion = +ve |
| Starting limb position | GHJ neutral, maximum elbow extension, forearm supination. |
| End limb position | Maximum elbow flexion, forearm supination. |
| Other considerations | To differentiate between the long, lateral and medial heads of the triceps brachii, bring the GHJ into 90 ̊ of flexion. Palpate to differentiate between the three heads of triceps brachii. Each head of the triceps brachii has a different pattern of force and activity during different shoulder elevations. The long head contributes to elbow extension more at shoulder elevation and the medial head takes over at > 90° of shoulder elevation. |
Goniometer landmarks
START:Control
Starting position: 10° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm

FINISH:Control
Finishing position(R2): 150° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
Control - Lateral view

START:Patient
Starting position: 0° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm

FINISH:Patient
Finishing position(R2): 150° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm

REACTION:Patient
Angle of muscle reaction (R1): 90° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
Spasticity angle = 60°
Patient - Lateral view
Triceps Brachii Medial Head
Elbow Extensors
| Triceps Brachii Medial Head | |
|---|---|
| Action | Extension at elbow. |
| Origin | Dorsal surface of shaft of the humerus, below groove for the radial nerve. |
| Insertion | Via a common tendon, the three heads of triceps brachii insert into the dorsal aspect of the olecranon of the ulna. |
| Innervation | Radial nerve (C7, C8, T1). |
| Injection site | Three fingerbreadths proximal to the medial epicondyle of the humerus. |
| Tardieu Testing | |
| Patient position | Sitting, with the scapula and head of the humerus supported. |
| Measurement considerations | Maximum elbow flexion = approximately 145 ̊ Full extension = 0 ̊ Flexion = +ve |
| Starting limb position | GHJ neutral, maximum elbow extension, forearm supination. |
| End limb position | Maximum elbow flexion, forearm supination. |
| Other considerations | To differentiate between long, lateral and medial heads of the triceps brachii, bring the GHJ into 90 ̊ of flexion. Palpate to differentiate between the three heads of triceps brachii. Each head of the triceps brachii has a different pattern of force and activity during different shoulder elevations. The long head contributes to elbow extension more at shoulder elevation and the medial head takes over at > 90° of shoulder elevation. |
Goniometer landmarks
START:Control
Starting position: 10° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
FINISH:Control
Finishing position(R2): 150° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
Control - Lateral view
START:Patient
Starting position: 0° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
FINISH:Patient
Finishing position(R2): 150° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
REACTION:Patient
Angle of muscle reaction (R1): 90° flexionStationary arm: humerus
Axis: elbow joint
Moving arm: forearm
Spasticity angle = 60°
Patient - Lateral view
Pronator Teres
Forearm Pronators
| Pronator Teres | |
|---|---|
| Action | Pronation of forearm. Assists with elbow flexion. |
| Origin | Common flexor tendon, medial supracondylar ridge of the humerus and the coronoid process of the ulna. |
| Insertion | Midway along the lateral surface of the radius. |
| Innervation | Median nerve (C6, C7). |
| Notes | Pronator quadratus is the prime mover in pronation. It receives help from pronator teres during rapid pronation. |
| Tardieu Testing | |
| Patient position | Sitting. |
| Measurement considerations | Neutral rotation = 0° (mid-prone) Supination = +ve Pronation = -ve |
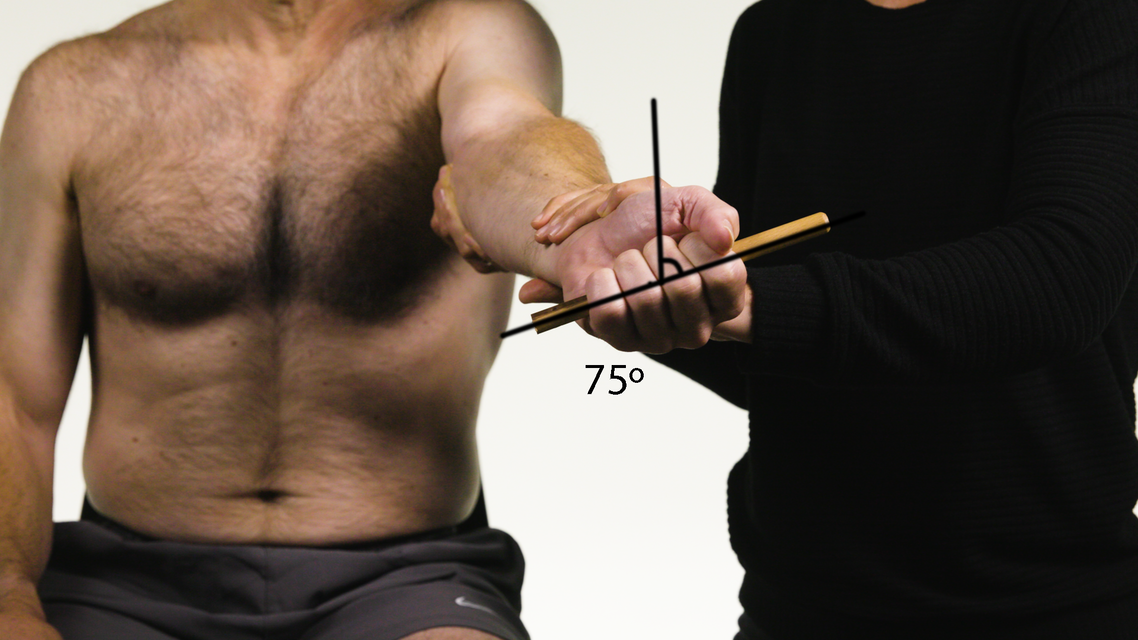
| Starting limb position | Maximum elbow extension, with forearm in full pronation and hand gripping a pen, if possible. |
| End limb position | Maximum forearm supination with elbow extended. |
| Other considerations | Hold the elbow in flexed position and straighten slowly. If the forearm pronates, pronator teres may have more spasticity than pronator quadratus. If the patient is unable to maintain elbow extension while supinating the forearm (for example, the elbow flexes), this is indicative of pronator teres spasticity. |
Goniometer landmarks

START:Control
Starting position: -90° supinationStationary arm: vertical
Axis: long axis of the forearm
Moving arm: stick/pen
FINISH:Control
Finishing position(R2): 75° supinationStationary arm: vertical
Axis: long axis of the forearm
Moving arm: stick/pen
Control - Lateral view
Control - Coronal (front) view

START:Patient
Starting position: -75° supinationStationary arm: vertical
Axis: long axis of the forearm
Moving arm: stick/pen

FINISH:Patient
Finishing position(R2): 45° supinationStationary arm: vertical
Axis: long axis of the forearm
Moving arm: stick/pen

REACTION:Patient
Angle of muscle reaction (R1): 0° supinationStationary arm: vertical
Axis: long axis of the forearm
Moving arm: stick/pen
Spasticity angle = 45°
Patient - Lateral view
Patient - Coronal (front) view
Pronator Quadratus
Forearm Pronators
| Pronator Quadratus | |
|---|---|
| Action | Pronation of forearm. |
| Origin | Medial, anterior surface of the ulna. |
| Insertion | Lateral, anterior surface of the radius. |
| Innervation | Median nerve (anterior interosseous nerve) (C8, T1). |
| Notes | Pronator quadratus is the prime mover in pronation and receives help from pronator teres during rapid pronation. |
| Tardieu Testing | |
| Patient position | Sitting. |
| Measurement considerations | Neutral rotation = 0° (mid-prone) Supination = +ve Pronation = -ve |
| Starting limb position | Elbow flexed to 90° with forearm in full pronation and hand gripping a pen, if possible. |
| End limb position | Elbow flexed to 90° with maximum forearm supination. |
| Other considerations | Hold the elbow in flexed position and straighten slowly. If the forearm pronates, pronator teres may have more spasticity than pronator quadratus. If the patient is unable to maintain elbow extension while supinating the forearm (for example, the elbow flexes), this is indicative of pronator teres spasticity. |
Goniometer landmarks

START:Control
Starting position: -85° supinationStationary arm: vertical
Axis: long axis of the forearm
Moving arm: stick/pen
FINISH:Control
Finishing position(R2): 80° supinationStationary arm: vertical
Axis: long axis of the forearm
Moving arm: stick/pen
Control - Lateral view
Control - Coronal (front) view
START:Patient
Starting position: -80° supinationStationary arm: vertical
Axis: long axis of the forearm
Moving arm: stick/pen
FINISH:Patient
Finishing position(R2): 30° supinationStationary arm: vertical
Axis: long axis of the forearm
Moving arm: stick/pen

REACTION:Patient
Angle of muscle reaction (R1): 0° supinationStationary arm: vertical
Axis: long axis of the forearm
Moving arm: stick/pen
Spasticity angle = 30°
Patient - Lateral view
Patient - Coronal (front) view
Flexor Carpi Radialis
Wrist Flexors
| Flexor Carpi Radialis | |
|---|---|
| Action | Flexion at wrist. |
| Origin | Common flexor tendon, medial epicondyle of the humerus and coronoid process of the ulna. |
| Insertion | FCR: base of 2nd and 3rd metacarpal. FCU: pisiform, hamate and 5th metacarpal. |
| Innervation | FCR: median nerve (C6, C7, C8). FCU: ulnar nerve (C8 and T1). |
| Notes | Observe hand posture to aid clinical decision making. FCU is a stronger wrist flexor than FCR and the power generator for manual labour. |
| Tardieu Testing | |
| Patient position | Sitting. |
| Measurement considerations | Neutral wrist extension = 0 ̊ Flexion = -ve Extension = +ve |
| Starting limb position | Fingers/thumb fully flexed to reduce impact of finger flexors on wrist. |
| End limb position | Fingers/thumb maintained in flexion, wrist extended as much as possible. |
| Other considerations | The goniometer is placed on the ulnar side of the wrist. It can differentiate between FCU and FCR by the amount of measured deviation, however, the Modified Tardieu score does not differentiate between these two muscles. |
Goniometer landmarks
 and Flexor Carpi Ulnaris (FCU) 2.png)
START:Control
Starting position: -40° extensionStationary arm: forearm
Axis: wrist joint
Moving arm: metacarpals
 and Flexor Carpi Ulnaris (FCU) 3.png)
FINISH:Control
Finishing position(R2): 65° extensionStationary arm: forearm
Axis: wrist joint
Moving arm: metacarpals
Control - Lateral view
 and Flexor Carpi Ulnaris (FCU) 2.png)
START:Patient
Starting position: -30° extensionStationary arm: forearm
Axis: wrist joint
Moving arm: metacarpals
 and Flexor Carpi Ulnaris (FCU) 3.png)
FINISH:Patient
Finishing position(R2): 20° extensionStationary arm: forearm
Axis: wrist joint
Moving arm: metacarpals
 and Flexor Carpi Ulnaris (FCU) 5.png)
REACTION:Patient
Angle of muscle reaction (R1): -10° extensionStationary arm: forearm
Axis: wrist joint
Moving arm: metacarpals
Spasticity angle = 30°
Patient - Lateral view
Flexor Carpi Ulnaris
Wrist Flexors
| Flexor Carpi Ulnaris | |
|---|---|
| Action | Flexion at wrist. |
| Origin | Common flexor tendon, medial epicondyle of the humerus and coronoid process of the ulna. |
| Insertion | FCR: base of 2nd and 3rd metacarpal. FCU: pisiform, hamate and 5th metacarpal. |
| Innervation | FCR: median nerve (C6, C7, C8). FCU: ulnar nerve (C8 and T1). |
| Notes | Observe hand posture to aid clinical decision making. FCU is a stronger wrist flexor than FCR and the power generator for manual labour. |
| Tardieu Testing | |
| Patient position | Sitting. |
| Measurement considerations | Neutral wrist extension = 0 ̊ Flexion = -ve Extension = +ve |
| Starting limb position | Fingers/thumb fully flexed to reduce impact of finger flexors on wrist. |
| End limb position | Fingers/thumb maintained in flexion, wrist extended as much as possible. |
| Other considerations | The goniometer is placed on the ulnar side of the wrist. It can differentiate between FCU and FCR by the amount of measured deviation, however, the Modified Tardieu score does not differentiate between these two muscles. |
Goniometer landmarks
START:Control
Starting position: -40° extensionStationary arm: forearm
Axis: wrist joint
Moving arm: metacarpals
FINISH:Control
Finishing position(R2): 65° extensionStationary arm: forearm
Axis: wrist joint
Moving arm: metacarpals
Control - Lateral view
START:Patient
Starting position: -30° extensionStationary arm: forearm
Axis: wrist joint
Moving arm: metacarpals
FINISH:Patient
Finishing position(R2): 20° extensionStationary arm: forearm
Axis: wrist joint
Moving arm: metacarpals
REACTION:Patient
Angle of muscle reaction (R1): -10° extensionStationary arm: forearm
Axis: wrist joint
Moving arm: metacarpals
Spasticity angle = 30°
Patient - Lateral view
Flexor Digitorum Superficialis
Finger Flexors
| Flexor Digitorum Superficialis | |
|---|---|
| Action | Flexion of the proximal interphalangeal (PIP) joint of the fingers. |
| Origin | Common flexor tendon, the medial epicondyle of the humerus and the coronoid process of the ulna. |
| Insertion | Bases of middle phalanges of digits 2 to 5. |
| Innervation | Median nerve (C7, C8, T1). |
| Tardieu Testing | |
| Patient position | Sitting. |
| Measurement considerations | Full DIP and PIP joint extension = 0 ̊ Flexion = -ve Hyperextension = +ve |
| Starting limb position | Wrist in 30° extension, if possible. MCP joints in neutral position, DIP joints extended, PIP joints in maximum flexion (approximately 130°). |
| End limb position | Wrist and MCP joints unchanged, PIP joints in as much extension as possible. |
| Other considerations | Stabilise DIP joints and MCP joints when moving PIP joints through passive range of movement. The fingers can be tested individually, as it is possible to isolate digit injection under ultrasound. Note, with respect to resting hand position, if FDS is involved, look for PIP flexion and DIP extension. |
Goniometer landmarks
 2.png)
START:Control
Starting position: -90° extensionStationary arm: proximal phalanx
Axis: 1st interphalangeal joint
Moving arm: middle phalanx
 3.png)
FINISH:Control
Finishing position(R2): 0° extensionStationary arm: proximal phalanx
Axis: 1st interphalangeal joint
Moving arm: middle phalanx
Control - Lateral view
Control - Aerial view
 2.png)
START:Patient
Starting position: -85° extensionStationary arm: proximal phalanx
Axis: 1st interphalangeal joint
Moving arm: middle phalanx
 3.png)
FINISH:Patient
Finishing position(R2): 0° extensionStationary arm: proximal phalanx
Axis: 1st interphalangeal joint
Moving arm: middle phalanx
 5.png)
REACTION:Patient
Angle of muscle reaction (R1): -70° extensionStationary arm: proximal phalanx
Axis: 1st interphalangeal joint
Moving arm: middle phalanx
Spasticity angle = 70°
Patient - Lateral view
Patient - Aerial view
Flexor Digitorum Profundus
Finger Flexors
| Flexor Digitorum Profundus | |
|---|---|
| Action | Flexion of distal phalanx of fingers. |
| Origin | Upper 3⁄4 of volar and medial aspects of the ulna. |
| Insertion | Bases of distal phalanges of digits 2 to 5. |
| Innervation | Median nerve (medial digits) / ulnar nerve (lateral digits) C7, C8, T1. |
| Notes | Ulnar 2 digits more superficial, medial 2 digits deeper. |
| Tardieu Testing | |
| Patient position | Sitting. |
| Measurement considerations | Full DIP extension = 0 ̊ Flexion = -ve Hyperextension = +ve |
| Starting limb position | Wrist in 30° extension, if possible. MCP joints in neutral, PIP joints in neutral and DIP joints in maximum flexion (approximately 90°). |
| End limb position | Wrist in 30° extension, if possible. MCP joints in neutral, PIP joints in neutral and DIP joints in as much extension as possible. |
| Other considerations | It may be difficult to maintain all other joints in a stable position, however, if the clinician can observe DIP joint flexion at the onset of measurement, this indicates tightness in the FDP. Note if the fingernails are digging into the palm at the onset of assessment. This may also indicate FDP spasticity. |
Goniometer landmarks
 2.png)
START:Control
Starting position: -60° extensionStationary arm: middle phalanx
Axis: 2nd interphalangeal joint
Moving arm: distal phalanx
 3.png)
FINISH:Control
Finishing position(R2): 0° extensionStationary arm: middle phalanx
Axis: 2nd interphalangeal joint
Moving arm: distal phalanx
Control - Lateral view
Control - Aerial view
 2.png)
START:Patient
Starting position: -85° extensionStationary arm: middle phalanx
Axis: 2nd interphalangeal joint
Moving arm: distal phalanx
 3.png)
FINISH:Patient
Finishing position(R2): 0° extensionStationary arm: middle phalanx
Axis: 2nd interphalangeal joint
Moving arm: distal phalanx
 5.png)
REACTION:Patient
Angle of muscle reaction (R1): -25° extensionStationary arm: middle phalanx
Axis: 2nd interphalangeal joint
Moving arm: distal phalanx
Spasticity angle = 25°
Patient - Lateral view
Patient - Aerial view
Flexor Pollicis Longus
Thumb Muscles
| Flexor Pollicis Longus | |
|---|---|
| Action | Flexion of the distal phalanx of the thumb. |
| Origin | Anterior surface of the body of the radius, from bicipital tuberosity to attachment of pronator quadratus and interosseous membrane. |
| Insertion | Anterior surface of base of the distal phalanx of the thumb. |
| Innervation | Anterior interosseous nerve, median nerve (C7, C8, T1). |
| Tardieu Testing | |
| Patient position | Sitting. |
| Measurement considerations | Flexion = -ve Full extension = 0° Hyperextension = +ve |
| Starting limb position | Wrist in 30° extension if possible, MCP joint in full extension. IP joint is measured in full flexion (approximately 80°). |
| End limb position | Wrist in 30° extension if possible, maintain MCP joint in extension, maximum IP joint extension. |
| Other considerations | Stabilise the thumb MCP joint when measuring FPL, to stabilise the joint in extension. |
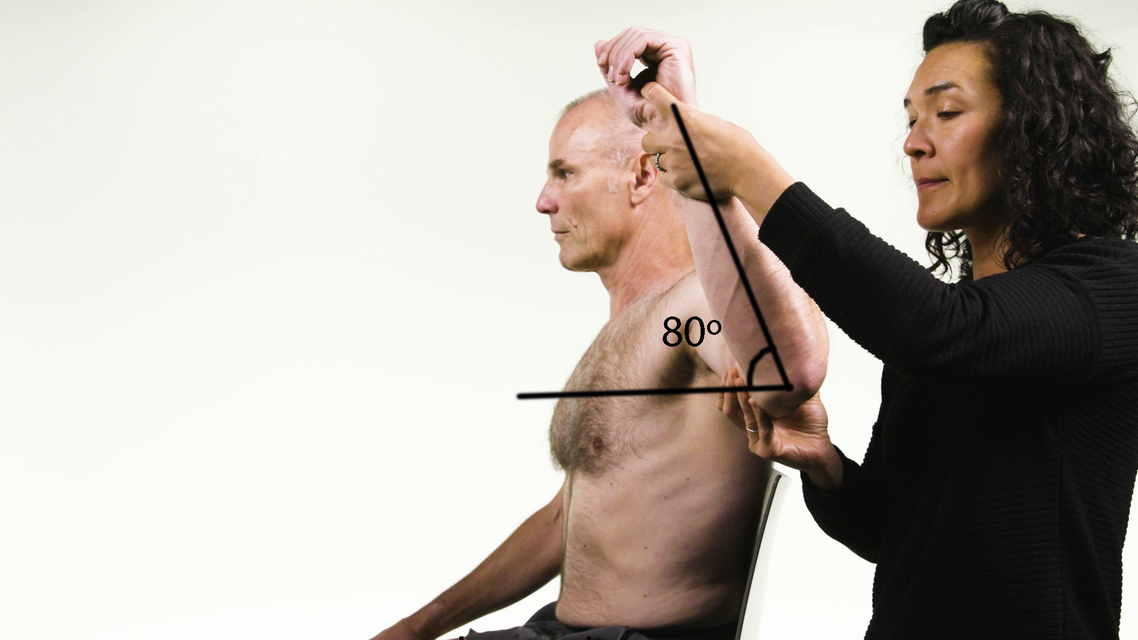
Goniometer landmarks
 2.png)
START:Control
Starting position: -50° extensionStationary arm: proximal phalanx
Axis: 1st interphalangeal joint
Moving arm: distal phalanx
 3.png)
FINISH:Control
Finishing position(R2): 0° extensionStationary arm: proximal phalanx
Axis: 1st interphalangeal joint
Moving arm: distal phalanx
Control - Lateral view
 2.png)
START:Patient
Starting position: -90° extensionStationary arm: proximal phalanx
Axis: 1st interphalangeal joint
Moving arm: distal phalanx
 3.png)
FINISH:Patient
Finishing position(R2): 0° extensionStationary arm: proximal phalanx
Axis: 1st interphalangeal joint
Moving arm: distal phalanx
 5.png)
REACTION:Patient
Angle of muscle reaction (R1): -80° extensionStationary arm: proximal phalanx
Axis: 1st interphalangeal joint
Moving arm: distal phalanx
Spasticity angle = 80°
Patient - Lateral view
Flexor Pollicis Brevis
Thumb Muscles
| Flexor Pollicis Brevis | |
|---|---|
| Action | Flexion of MCP joint of thumb. |
| Origin | Deep head: trapezoid and capitate. Superficial head: ridge of trapezium and flexor retinaculum. |
| Insertion | Radial side of base of the proximal phalanx of the thumb. |
| Innervation | Deep head: Ulnar nerve. Superficial head: Median nerve. |
| Tardieu Testing | |
| Patient position | Sitting. |
| Measurement considerations | Flexion = -ve Full extension = 0° Extension = +ve |
| Starting limb position | Wrist in neutral, MCP in full flexion. DIP joint in full extension |
| End limb position | Wrist in neutral, maximum MCP extension. |
| Other considerations | Hold the 1st metacarpal joint when measuring FPB to stabilise it when extending the MCP joint. Stabilise the IP joint during testing, to maintain joint extension. |
Goniometer landmarks
 2.png)
START:Control
Starting position: -70° extensionStationary arm: 1st metacarpal
Axis: 1st metacarpophalangeal joint
Moving arm: proximal phalanx
 3.png)
FINISH:Control
Finishing position(R2): 0° extensionStationary arm: 1st metacarpal
Axis: 1st metacarpophalangeal joint
Moving arm: proximal phalanx
Control - Lateral view
 2.png)
START:Patient
Starting position: -60° extensionStationary arm: 1st metacarpal
Axis: 1st metacarpophalangeal joint
Moving arm: proximal phalanx
 3.png)
FINISH:Patient
Finishing position(R2): 0° extensionStationary arm: 1st metacarpal
Axis: 1st metacarpophalangeal joint
Moving arm: proximal phalanx
 5.png)
REACTION:Patient
Angle of muscle reaction (R1): -40° extensionStationary arm: 1st metacarpal
Axis: 1st metacarpophalangeal joint
Moving arm: proximal phalanx
Spasticity angle = 40°
Patient - Lateral view
Adductor Pollicis
Thumb Muscles
| Adductor Pollicis | |
|---|---|
| Action | Adduction of the CMC joint of the thumb |
| Origin | Transverse head: Palmar base of metacarpal bone 3. Oblique head: Capitate bone, palmar bases of metacarpal bones 2 and 3. |
| Insertion | Radial side of base of the proximal phalanx of the thumb. |
| Innervation | Deep branch of ulnar nerve (C8, T1). |
| Tardieu Testing | |
| Patient position | Sitting. |
| Measurement considerations | Abduction +ve Neutral = 0° Adduction =-ve |
| Starting limb position | Wrist in neutral. CMC and MCP in full adduction. |
| End limb position | Wrist in neutral, maximum CMC and MPC abduction. |
| Other considerations | Most powerful intrinsic muscle of the hand. Essential for functions that require pinching and gripping. Additionally, the adductor pollicis aids the later stages of opposition of the thumb. |
Goniometer landmarks

START:Control
Starting position: 0° abductionStationary arm: 2nd metacarpal
Axis: 1st carpo-metacarpal joint
Moving arm: 1st metacarpal
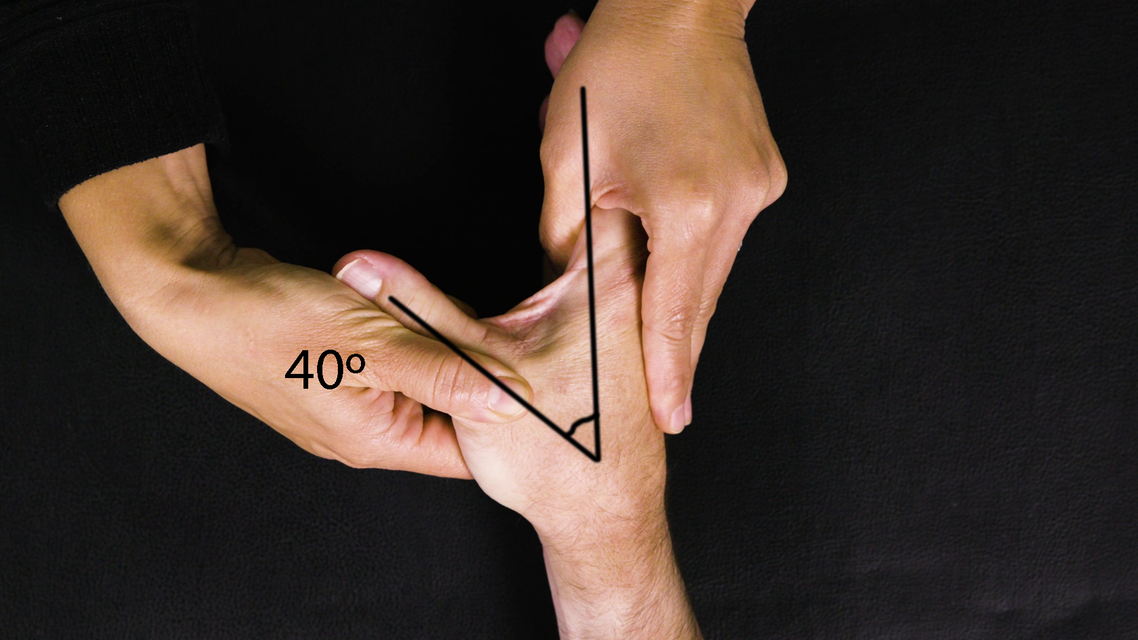
FINISH:Control
Finishing position(R2): 40° abductionStationary arm: 2nd metacarpal
Axis: 1st carpo-metacarpal joint
Moving arm: 1st metacarpal
Control - Aerial view
START:Patient
Starting position: 0° abductionStationary arm: 2nd metacarpal
Axis: 1st carpo-metacarpal joint
Moving arm: 1st metacarpal
FINISH:Patient
Finishing position(R2): 40° abductionStationary arm: 2nd metacarpal
Axis: 1st carpo-metacarpal joint
Moving arm: 1st metacarpal
REACTION:Patient
Angle of muscle reaction (R1): 20° abductionStationary arm: 2nd metacarpal
Axis: 1st carpo-metacarpal joint
Moving arm: 1st metacarpal
Spasticity angle = 20°
Patient - Aerial view
Intrinsic Finger Flexors (lumbricals)
Hand Muscles
| Intrinsic Finger Flexors (lumbricals) | |
|---|---|
| Action | Flexion at MCP joints. |
| Origin | Radial aspect of tendon sheath of FDP. |
| Insertion | Extensor expansion on dorsum of proximal phalanges. |
| Innervation | Digits 1 and 2 - median nerve (C8, T1). Digits 3 and 4 - ulnar nerve (C8, T1). |
| Tardieu Testing | |
| Patient position | Sitting. |
| Measurement considerations | MCP extension = +ve MCP flexion = -ve |
| Starting limb position | Wrist in neutral, PIP and DIP joints in full flexion, MCP joints in full flexion (approximately 90°). |
| End limb position | Maintain wrist in neutral with PIP and DIP joints fully flexed, maximum MCP joint extension. |
| Other considerations | Measure MCP joint angle from ulnar side of hand. |
Goniometer landmarks
 2.png)
START:Control
Starting position: -80° extensionStationary arm: 5th metacarpal
Axis: 5th metacarpophalangeal joint
Moving arm: proximal phalanx
 3.png)
FINISH:Control
Finishing position(R2): 15° extensionStationary arm: 5th metacarpal
Axis: 5th metacarpophalangeal joint
Moving arm: proximal phalanx
Control - Lateral view
 2.png)
START:Patient
Starting position: -90° extensionStationary arm: 5th metacarpal
Axis: 5th metacarpophalangeal joint
Moving arm: proximal phalanx
 3.png)
FINISH:Patient
Finishing position(R2): -10° extensionStationary arm: 5th metacarpal
Axis: 5th metacarpophalangeal joint
Moving arm: proximal phalanx
 5.png)
REACTION:Patient
Angle of muscle reaction (R1): -40° extensionStationary arm: 5th metacarpal
Axis: 5th metacarpophalangeal joint
Moving arm: proximal phalanx
Spasticity angle = 30°
Patient - Lateral view
Adductor Brevis
Hip Adductors
| Adductor Brevis | |
|---|---|
| Action | Adduction at the hip joint. |
| Origin | Inferior pubic ramus. |
| Insertion | Pectineal line and linea aspera (deep to the pectineus and adductor longus). |
| Innervation | Anterior division of the obturator nerve. |
| Differential diagnosis | Tightness of the secondary hip flexors, such as adductor brevis, would, in theory, contribute to an excessive anterior pelvic tilt. |
| Notes | Due to the bulk of adductors and the quantity of toxin needed to be injected, if all adductors are indicated, consider an obturator nerve block. |
| Tardieu Testing | |
| Patient position | Supine, with hip and knee neutral. |
| Measurement considerations | Anatomical midline position of the hip = 0° Adduction (towards midline) = -ve Abduction (away from midline) = +ve |
| Starting limb position | Maximum hip adduction. |
| End limb position | Maximum hip abduction. |
| Phase of gait cycle | May cause hip adduction in stance or swing phase. |
| Gait cycle observation | Scissoring gait. |
| Other considerations | Differentiate between adductor brevis, longus and magnus with palpation. Often, another person is needed to stabilise the opposite thigh/pelvis during testing. The adductors help to stabilise lateral movement of the trunk when standing or balancing on an unstable surface, therefore, before injecting, the clinician must consider this role in the presence of severe lower limb weakness. |
Goniometer landmarks
START:Control
Starting position: -10° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur

FINISH:Control
Finishing position(R2): 25° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur
Control - Coronal (front) view

START:Patient
Starting position: -10° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur

FINISH:Patient
Finishing position(R2): 15° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur

REACTION:Patient
Angle of muscle reaction (R1): 5° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur
Spasticity angle = 10°
Patient - Coronal (front) view
Adductor Longus
Hip Adductors
| Adductor Longus | |
|---|---|
| Action | Adduction, flexion and medial rotation of the hip joint. |
| Origin | Medial portion of the superior pubic ramus. |
| Insertion | Middle third of linea aspera of the femur. |
| Innervation | Anterior division of the obturator nerve. |
| Differential diagnosis | The most anterior of the adductor group of muscles. Adductor longus is a large, flat muscle that covers adductor magnus and brevis. |
| Notes | Due to the bulk of adductors and quantity of toxin needed to be injected, if all adductors are indicated, consider an obturator nerve block. |
| Tardieu Testing | |
| Patient position | Supine, with hip and knee neutral. |
| Measurement considerations | Anatomical midline position of the hip = 0° Adduction (towards midline) = -ve Abduction (away from midline) = +ve |
| Starting limb position | Maximum hip adduction. |
| End limb position | Maximum hip abduction. |
| Phase of gait cycle | May cause hip adduction in stance or swing phase. |
| Gait cycle observation | Scissoring gait. |
| Other considerations | Differentiate between adductor brevis, longus and magnus with palpation. Often, another person is needed to stabilise the opposite thigh/pelvis during testing. The adductors help to stabilise lateral movement of the trunk when standing or balancing on an unstable surface, therefore, before injecting, the clinician must consider this role in the presence of severe lower limb weakness. |
Goniometer landmarks
START:Control
Starting position: -10° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur
FINISH:Control
Finishing position(R2): 25° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur
Control - Coronal (front) view
START:Patient
Starting position: -10° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur
FINISH:Patient
Finishing position(R2): 15° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur
REACTION:Patient
Angle of muscle reaction (R1): 5° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur
Spasticity angle = 10°
Patient - Coronal (front) view
Adductor Magnus
Hip Adductors
| Adductor Magnus | |
|---|---|
| Action | Adduction and extension of the femur (ischiocondylar part). |
| Origin | Ischiopubic ramus and ischial tuberosity. |
| Insertion | Linea aspera of the femur; the ischiocondylar part inserts on the adductor tubercle of the femur. |
| Innervation | Posterior division of the obturator nerve; tibial nerve (ischiocondylar part). |
| Differential diagnosis | The ischiocondylar part of adductor magnus is a hamstring muscle by embryonic origin and action, therefore, it is innervated by the tibial nerve. |
| Notes | Due to the bulk of adductors and the quantity of toxin needed to be injected, if all adductors are indicated, consider an obturator nerve block. |
| Tardieu Testing | |
| Patient position | Supine, with hip and knee neutral. |
| Measurement considerations | Anatomical midline position of the hip = 0° Adduction (towards midline) = -ve Abduction (away from midline) = +ve |
| Starting limb position | Maximum hip adduction. |
| End limb position | Maximum hip abduction. |
| Phase of gait cycle | May cause hip adduction in stance or swing phase. |
| Gait cycle observation | Scissoring gait. |
| Other considerations | Differentiate between adductor brevis, longus and magnus with palpation. Often, another person is needed to stabilise the opposite thigh/pelvis during testing. The adductors help to stabilise lateral movement of the trunk when standing or balancing on an unstable surface, therefore, before injecting, the clinician must consider this role in the presence of severe lower limb weakness. |
Goniometer landmarks
START:Control
Starting position: -10° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur
FINISH:Control
Finishing position(R2): 25° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur
Control - Coronal (front) view
START:Patient
Starting position: -10° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur
FINISH:Patient
Finishing position(R2): 15° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur
REACTION:Patient
Angle of muscle reaction (R1): 5° abductionStationary arm: midline
Axis: hip joint
Moving arm: femur
Spasticity angle = 10°
Patient - Coronal (front) view
Psoas Major
Hip Flexors
| Psoas Major | |
|---|---|
| Action | Hip flexion. |
| Origin | Bodies and transverse processes of lumbar vertebrae. |
| Insertion | Lesser trochanter of the femur (with iliacus) via iliopsoas tendon. |
| Innervation | Branches of the ventral primary rami of spinal nerves L2 to L4. |
| Tardieu Testing | |
| Patient position | Supine. |
| Measurement considerations | Neutral hip position = 0° Hip flexion = -ve Hip extension = +ve |
| Starting limb position | Maximum hip flexion with the pelvis on the edge of the plinth to allow for hip extension. Pelvis must remain in neutral during testing. |
| End limb position | Maximum hip extension, maintaining posterior tilt as much as possible. Speed is V2. |
| Phase of gait cycle | Flexes the hip from toe-off through to early swing. |
| Gait cycle observation | Excessive anterior pelvic tilt, increased lumbar lordosis and reduced hip extension in terminal stance. |
| Other considerations | Differentiate from rectus femoris by avoiding maximum knee flexion. |
Goniometer landmarks
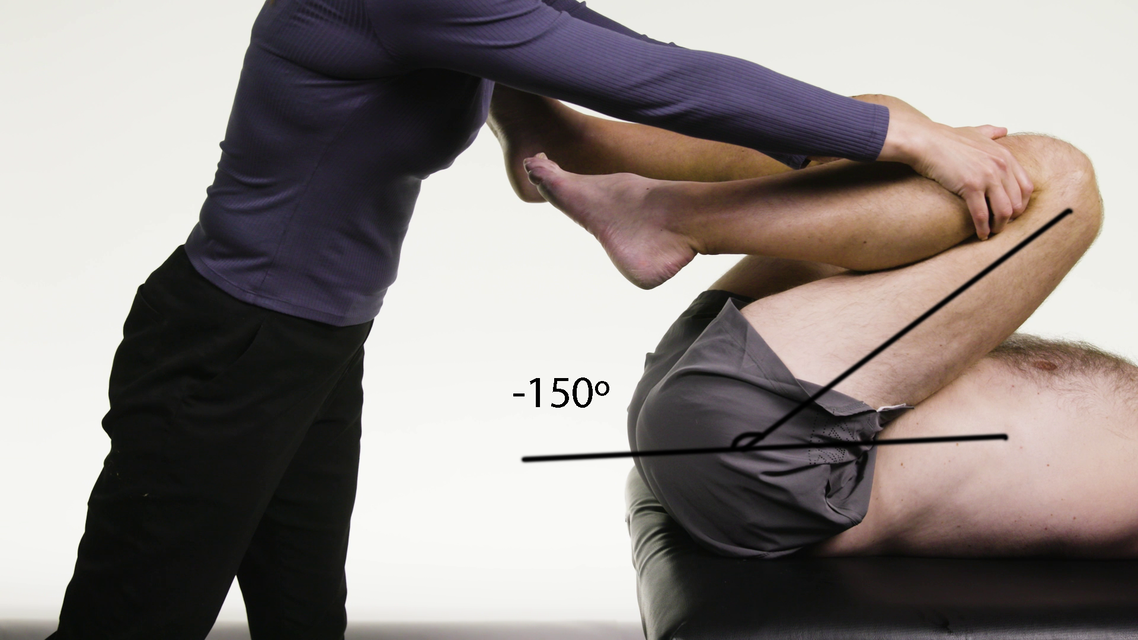
START:Control
Starting position: -150° extensionStationary arm: horizontal
Axis: hip joint
Moving arm: femur
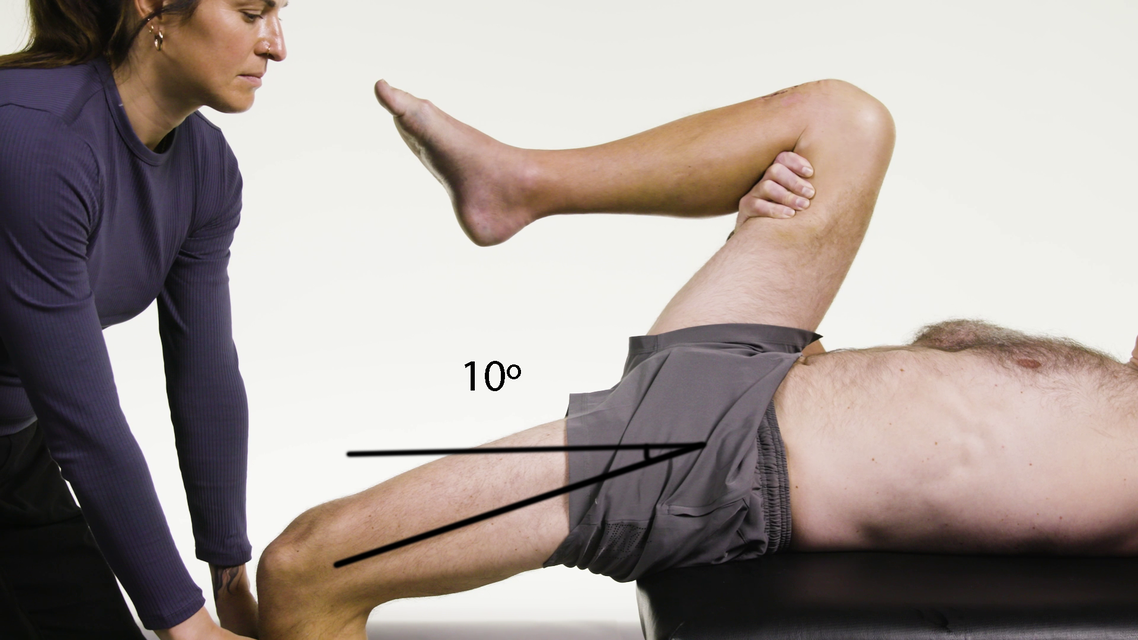
FINISH:Control
Finishing position(R2): 10° extensionStationary arm: horizontal
Axis: hip joint
Moving arm: femur
Control - Lateral view
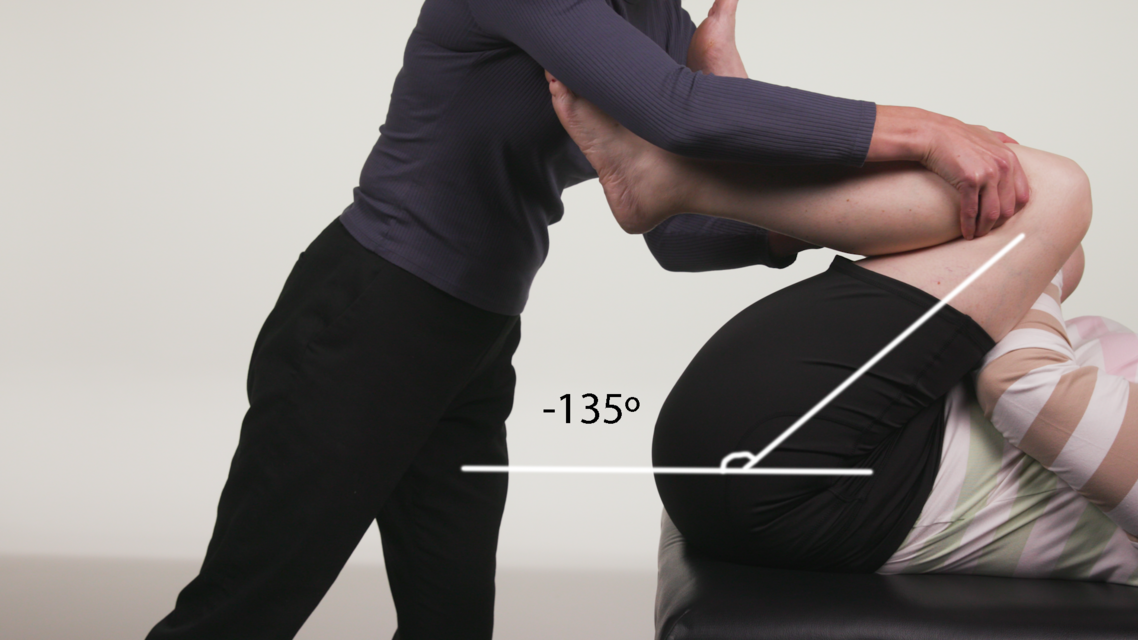
START:Patient
Starting position: -135° extensionStationary arm: horizontal
Axis: hip joint
Moving arm: femur
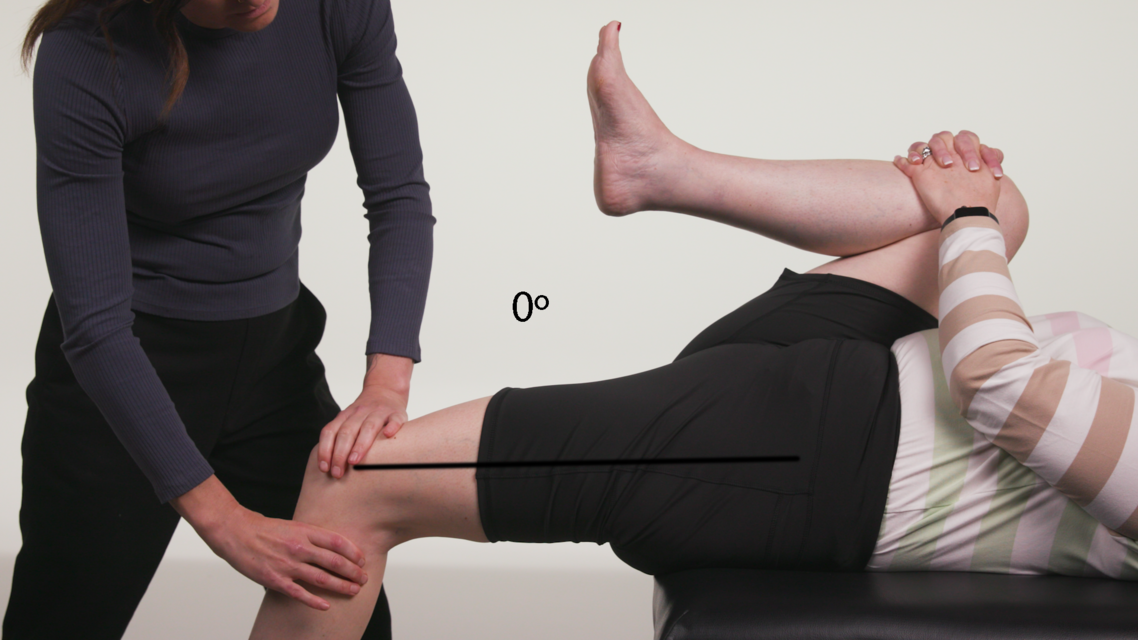
FINISH:Patient
Finishing position(R2): 0° extensionStationary arm: horizontal
Axis: hip joint
Moving arm: femur

REACTION:Patient
Angle of muscle reaction (R1): -25° extensionStationary arm: horizontal
Axis: hip joint
Moving arm: femur
Spasticity angle = 25°
Patient - Lateral view
Semimembranosus
Knee Flexors
| Semimembranosus | |
|---|---|
| Action | Hip extension, knee flexion. |
| Origin | Upper, outer surface of the ischial tuberosity. |
| Insertion | Medial condyle of the tibia. |
| Innervation | Tibial nerve. |
| Tardieu Testing | |
| Patient position | Supine. |
| Measurement considerations | Full knee extension = 0° Flexion = -ve Hyperextension = +ve |
| Starting limb position | Hip in 90° flexion, with maximum knee flexion. |
| End limb position | Hip in 90° flexion, with maximum knee extension. |
| Phase of gait cycle | The semimembranosus has two roles; firstly, to extend the hip in early stance and, secondly, to decelerate the tibia in late swing. |
| Gait cycle observation | Increased knee flexion in terminal swing and at initial contact. |
| Other considerations | Palpate to differentiate between the hamstrings. Medial to lateral: semimembranosus, semitendinosus and biceps femoris. Consider testing hamstrings in 30° to 40° hip flexion, to replicate hip position at late swing/early stance phase of gait. |
Goniometer landmarks

START:Control
Starting position: -150° extensionStationary arm: vertical
Axis: knee joint
Moving arm: tibia

FINISH:Control
Finishing position(R2): -5° extensionStationary arm: vertical
Axis: knee joint
Moving arm: tibia
Control - Lateral view

START:Patient
Starting position: -140° extensionStationary arm: vertical
Axis: knee joint
Moving arm: tibia
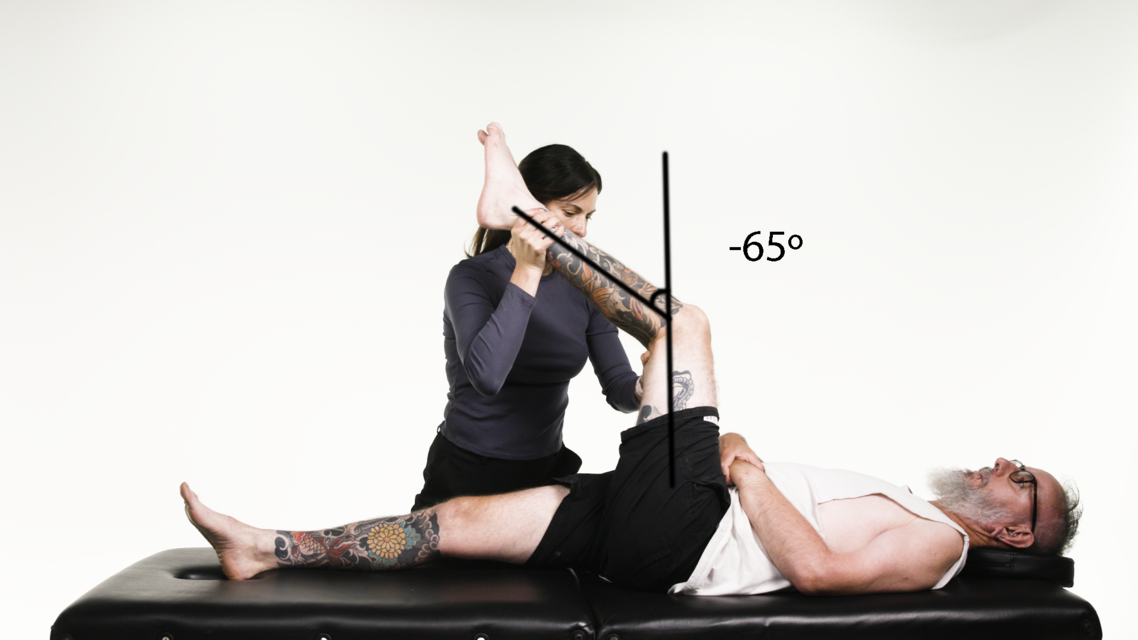
FINISH:Patient
Finishing position(R2): -65° extensionStationary arm: vertical
Axis: knee joint
Moving arm: tibia
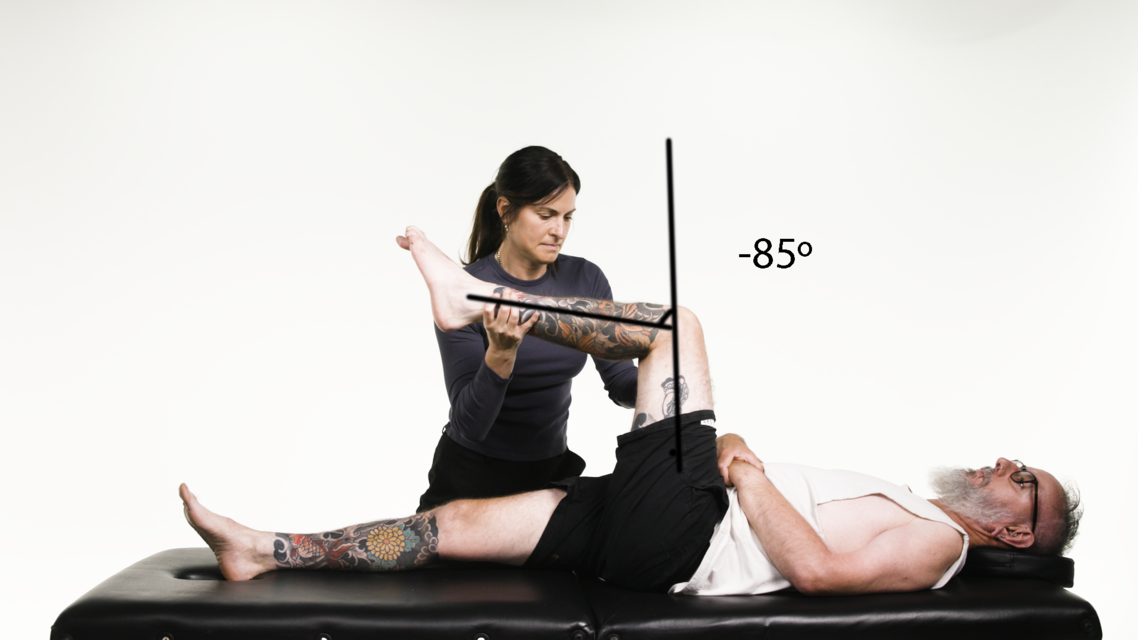
REACTION:Patient
Angle of muscle reaction (R1): -85° extensionStationary arm: vertical
Axis: knee joint
Moving arm: tibia
Spasticity angle = 20°
Patient - Lateral view
Semitendinosus
Knee Flexors
| Semitendinosus | |
|---|---|
| Action | Hip extension, knee flexion. |
| Origin | Ischial tuberosity (common tendon with biceps femoris). |
| Insertion | Medial surface of the tibia (via pes anserinus). |
| Innervation | Tibial nerve. |
| Differential diagnosis | Pes anserinus is the common insertion for the gracilis, sartorius, and semitendinosus muscles. |
| Tardieu Testing | |
| Patient position | Supine. |
| Measurement considerations | Full knee extension = 0° Flexion = -ve Hyperextension = +ve |
| Starting limb position | Hip in 90° flexion, with maximum knee flexion. |
| End limb position | Hip in 90° flexion, with maximum knee extension. |
| Phase of gait cycle | The semitendinosus has two roles; firstly, to extend the hip in early stance and, secondly, to decelerate the tibia in late swing. |
| Gait cycle observation | Increased knee flexion in terminal swing and at initial contact. |
| Other considerations | Palpate to differentiate between the hamstrings. Medial to lateral: semimembranosus, semitendinosus and biceps femoris. Consider testing hamstrings in 30° to 40° hip flexion to replicate hip position at late swing/early stance phase of gait. |
Goniometer landmarks
START:Control
Starting position: -150° extensionStationary arm: vertical
Axis: knee joint
Moving arm: tibia
FINISH:Control
Finishing position(R2): -5° extensionStationary arm: vertical
Axis: knee joint
Moving arm: tibia
Control - Lateral view
START:Patient
Starting position: -140° extensionStationary arm: vertical
Axis: knee joint
Moving arm: tibia
FINISH:Patient
Finishing position(R2): -65° extensionStationary arm: vertical
Axis: knee joint
Moving arm: tibia
REACTION:Patient
Angle of muscle reaction (R1): -85° extensionStationary arm: vertical
Axis: knee joint
Moving arm: tibia
Spasticity angle = 20°
Patient - Lateral view
Biceps Femoris
Knee Flexors
| Biceps Femoris | |
|---|---|
| Action | Hip extension, knee flexion. |
| Origin | Long head: ischial tuberosity. Short head: lateral lip of the linea aspera. |
| Insertion | Head of fibula and lateral condyle of the tibia. |
| Innervation | Long head: tibial nerve. Short head: common fibular (peroneal) nerve. |
| Differential diagnosis | The long head of biceps femoris has a secondary action of hip adduction which is important to consider in scissoring gait. |
| Tardieu Testing | |
| Patient position | Supine. Speed is V2. |
| Measurement considerations | Full knee extension = 0° Flexion = -ve Hyperextension = +ve |
| Starting limb position | Hip in 30° to 40° of flexion with maximum knee flexion. |
| End limb position | Hip in 30° to 40° of flexion with maximum knee extension. |
| Phase of gait cycle | The biceps femoris has two roles; firstly, to extend the hip in early stance (long head) and, secondly, to decelerate the tibia in late swing (both heads). |
| Gait cycle observation | Increased knee flexion in terminal swing and at initial contact. |
| Other considerations | Palpate to differentiate between the hamstrings. Medial to lateral: semimembranosus, semitendinosus and biceps femoris. Consider testing hamstrings in 30° to 40° hip flexion to replicate hip position at late swing/early stance phase of gait. |
Goniometer landmarks

START:Control
Starting position: -90° extensionStationary arm: femur
Axis: knee joint
Moving arm: tibia

FINISH:Control
Finishing position(R2): 0° extensionStationary arm: femur
Axis: knee joint
Moving arm: tibia
Control - Lateral view

START:Patient
Starting position: -130° extensionStationary arm: femur
Axis: knee joint
Moving arm: tibia

FINISH:Patient
Finishing position(R2): -65° extensionStationary arm: femur
Axis: knee joint
Moving arm: tibia
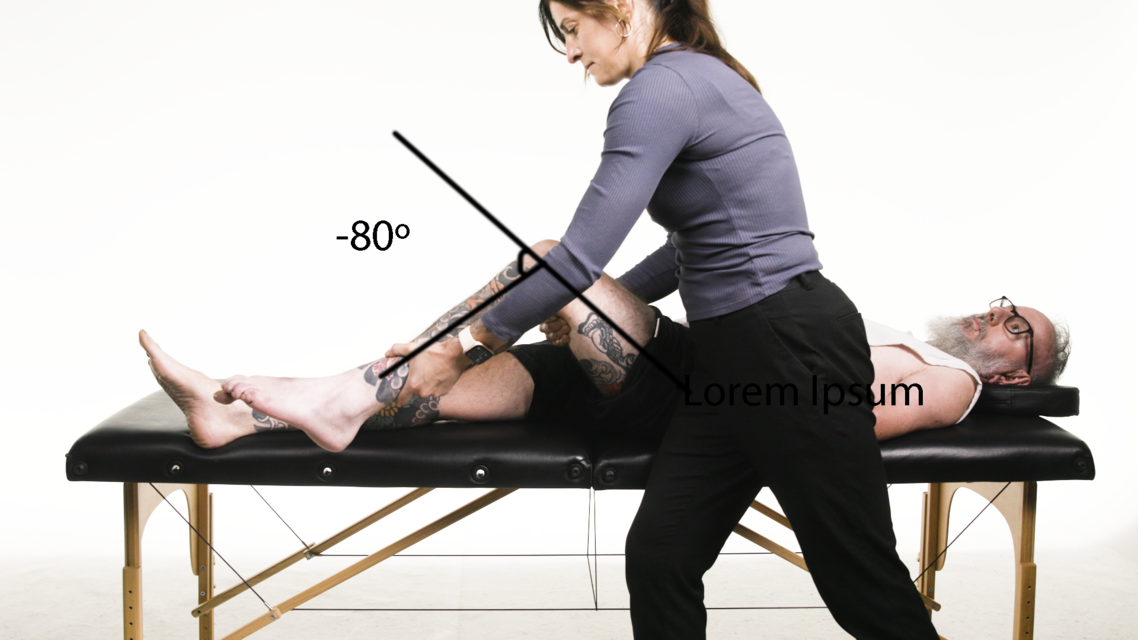
REACTION:Patient
Angle of muscle reaction (R1): -80° extensionStationary arm: femur
Axis: knee joint
Moving arm: tibia
Spasticity angle = 15°
Patient - Lateral view
Vastus Lateralis
Knee Extensors
| Vastus Lateralis | |
|---|---|
| Action | Knee extension. |
| Origin | Lateral lip of the linea aspera, greater trochanter and intertrochanteric line. |
| Insertion | Patella and medial patellar retinaculum. |
| Innervation | Femoral nerve. |
| Differential diagnosis | Differentiate from rectus femoris with hip extension. |
| Tardieu Testing | |
| Patient position | Sitting on the edge of the bed. |
| Measurement considerations | Full knee extension = 0° Flexion = +ve Extension = -ve |
| Starting limb position | Maximum knee extension. |
| End limb position | Drop leg and observe movement quality into flexion. Speed = V2 |
| Phase of gait cycle | Acts eccentrically in terminal stance and early swing, some support of extension in early stance, and stiff-legged gait in swing phase. |
| Gait cycle observation | May contribute to knee hyperextension in stance phase and stiff-legged gait in swing phase. |
| Other considerations | Differentiate from rectus femoris with hip extension. |
Goniometer landmarks
START:Control
Starting position: 0° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia

FINISH:Control
Finishing position(R2): 120° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
Control - Lateral view
START:Patient
Starting position: 5° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia

FINISH:Patient
Finishing position(R2): 125° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
REACTION:Patient
Angle of muscle reaction (R1): 55° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
Spasticity angle = 70°
Patient - Lateral view
Vastus Medialis
Knee Extensors
| Vastus Medialis | |
|---|---|
| Action | Knee extension. |
| Origin | Medial intermuscular septum, medial lip of the linea aspera, intertrochanteric line and tendon of adductor magnus. |
| Insertion | Patella and medial patellar retinaculum. |
| Innervation | Femoral nerve. |
| Differential diagnosis | Differentiate from rectus femoris with hip extension |
| Tardieu Testing | |
| Patient position | Sitting on the edge of the bed. |
| Measurement considerations | Full knee extension = 0° Flexion = +ve Extension = -ve |
| Starting limb position | Maximum knee extension. |
| End limb position | Drop leg and observe movement quality into flexion. Speed = V2. |
| Phase of gait cycle | Acts eccentrically in terminal stance and early swing. |
| Gait cycle observation | May contribute to knee hyperextension in stance phase and stiff-legged gait in swing phase. |
| Other considerations | Differentiate from rectus femoris with hip extension. |
Goniometer landmarks
START:Control
Starting position: 0° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
FINISH:Control
Finishing position(R2): 120° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
Control - Lateral view
START:Patient
Starting position: 5° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
FINISH:Patient
Finishing position(R2): 125° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
REACTION:Patient
Angle of muscle reaction (R1): 55° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
Spasticity angle = 70°
Patient - Lateral view
Vastus Intermedius
Knee Extensors
| Vastus Intermedius | |
|---|---|
| Action | Knee extension. |
| Origin | Anterior and lateral surface of the femur. |
| Insertion | Patella. |
| Innervation | Femoral nerve. |
| Differential diagnosis | Differentiate from rectus femoris with hip extension. |
| Tardieu Testing | |
| Patient position | Sitting on the edge of the bed. |
| Measurement considerations | Full knee extension = 0° Flexion = +ve Extension = -ve |
| Starting limb position | Maximum knee extension. |
| End limb position | Drop leg and observe movement quality into flexion. Speed = V2 |
| Phase of gait cycle | Acts eccentrically in terminal stance and early swing. |
| Gait cycle observation | May contribute to knee hyperextension in stance phase, and stiff-legged gait in swing phase. |
| Other considerations | Differentiate from rectus femoris with hip extension. |
Goniometer landmarks
START:Control
Starting position: 0° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
FINISH:Control
Finishing position(R2): 120° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
Control - Lateral view
START:Patient
Starting position: 5° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
FINISH:Patient
Finishing position(R2): 125° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
REACTION:Patient
Angle of muscle reaction (R1): 55° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
Spasticity angle = 70°
Patient - Lateral view
Rectus Femoris (prone)
Knee Extensors
| Rectus Femoris (prone) | |
|---|---|
| Action | Hip flexion, knee extension. |
| Origin | Straight head: anterior inferior iliac spine Reflected head: groove above the acetabulum. |
| Insertion | Patella and tibial tuberosity (via the patellar ligament). |
| Innervation | Femoral nerve. |
| Differential diagnosis | To differentiate from vasti muscles, have the patient sitting on the edge of the bed with 90° hip flexion. |
| Tardieu Testing | |
| Patient position | Prone is the standardised position for testing rectus femoris, however, the supine position can be used when the person is unable to lie prone. Prone: Pelvis neutral, hip neutral, knee extended. Bend knee quickly. Useful to monitor hip flexion or pelvic retraction during testing. Supine: Pelvis neutral, hip neutral, knee extended. Drop the lower leg over the side of the bed with gravity and support at the angle of catch or clonus. Useful for people unable to lie prone or on a small plinth. |
| Measurement considerations | Full knee extension = 0° Flexion = +ve Hyperextension = -ve |
| Starting limb position | Hip neutral, knee extended. |
| End limb position | Maximum knee flexion. |
| Phase of gait cycle | Acts eccentrically in terminal stance. |
| Gait cycle observation | Stiff-legged gait. May contribute to knee hyperextension in stance phase, and stiff-legged gait in swing phase. |
| Other considerations | To differentiate from vasti muscles, have the patient sitting on the edge of the bed with 90° hip flexion. |
Goniometer landmarks
START:Control
Starting position: 0° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia

FINISH:Control
Finishing position(R2): 130° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
Control - Lateral view
START:Patient
Starting position: 0° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia

FINISH:Patient
Finishing position(R2): 120° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia

REACTION:Patient
Angle of muscle reaction (R1): 65° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
Spasticity angle = 55°
Patient - Lateral view
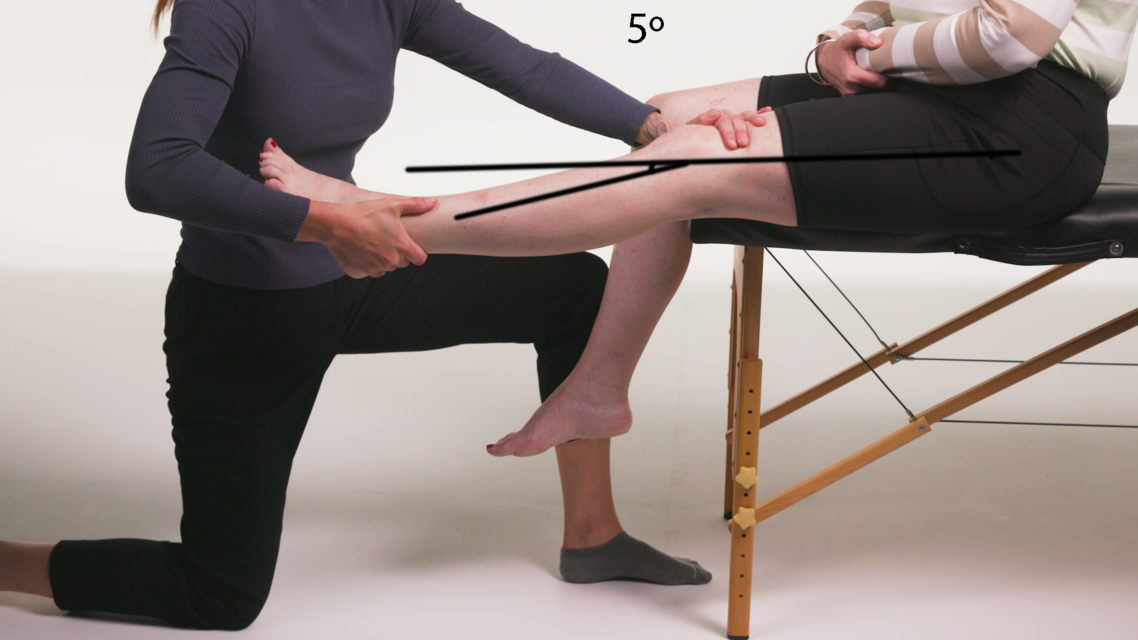
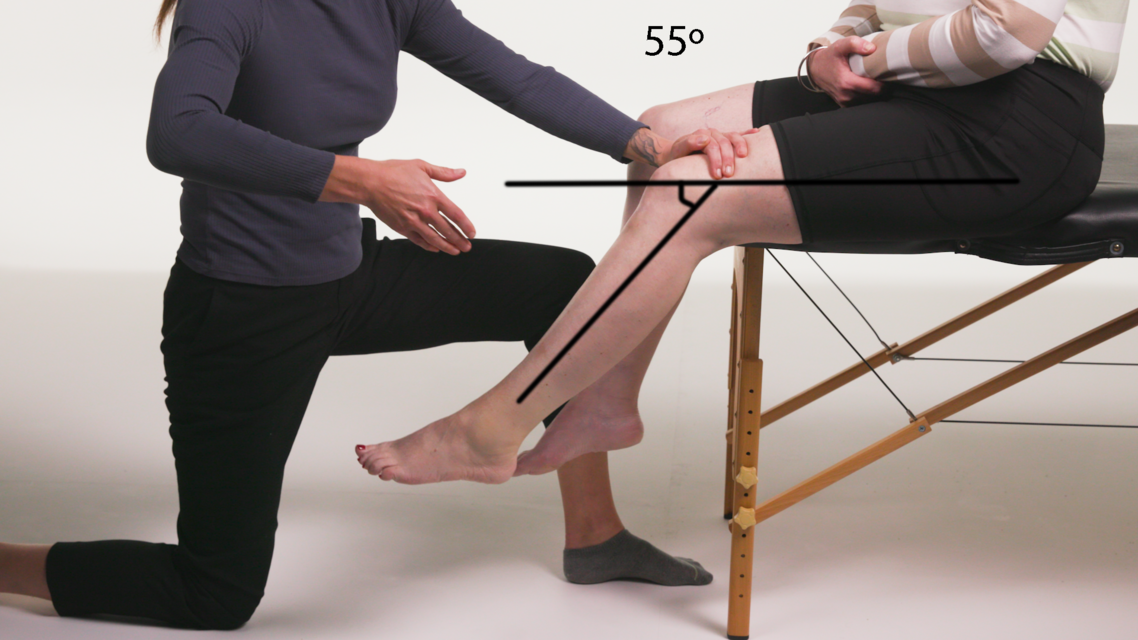
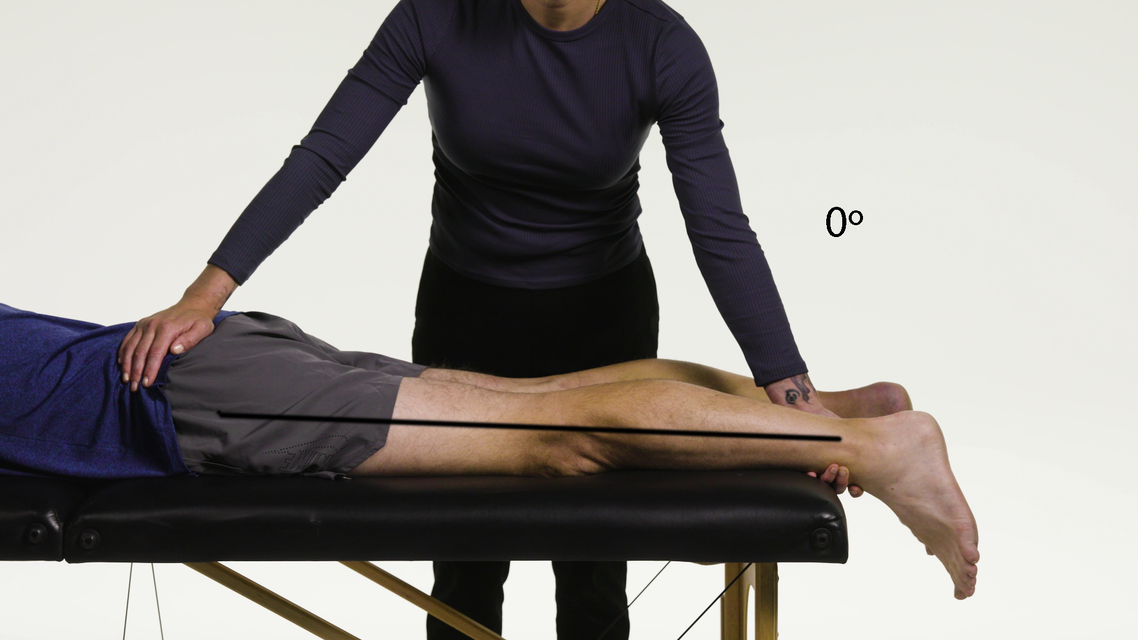
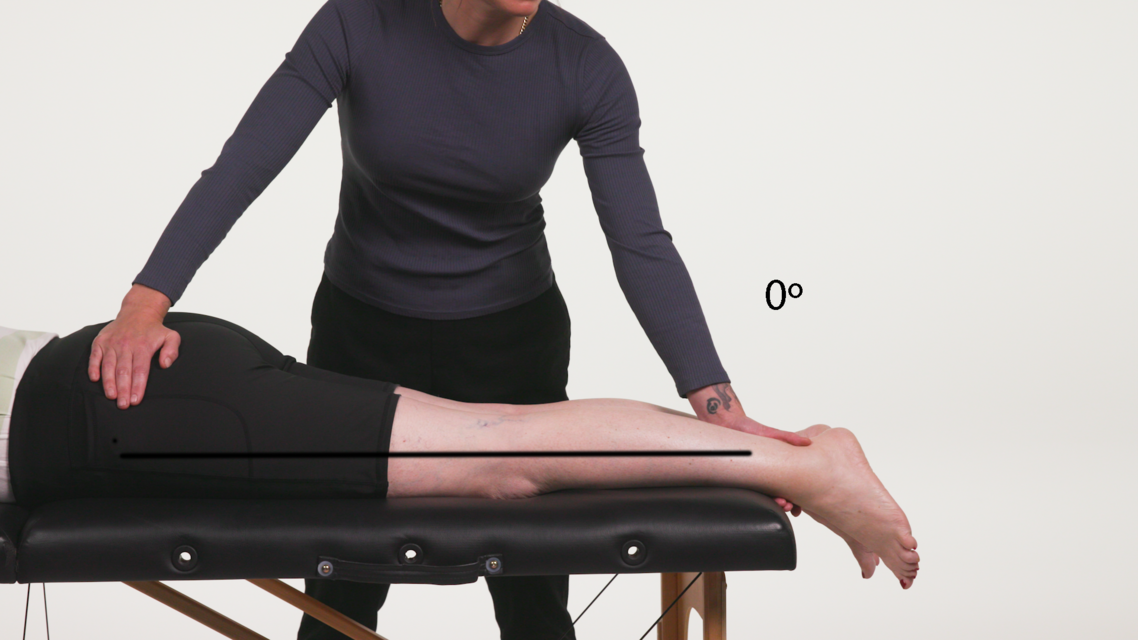
Rectus Femoris (supine)
Knee Extensors
| Rectus Femoris (supine) | |
|---|---|
| Action | Hip flexion, knee extension. |
| Origin | Straight head: anterior inferior iliac spine. Reflected head: groove above the acetabulum. |
| Insertion | Patella and tibial tuberosity (via the patellar ligament). |
| Innervation | Femoral nerve. |
| Differential diagnosis | To differentiate from vasti muscles, have the patient sitting on the edge of the bed with 90° hip flexion. |
| Tardieu Testing | |
| Patient position | The supine position is used when the person is unable to lie prone, however prone is the standardised position for testing rectus femoris. |
| Supine | Pelvis neutral, hip neutral, knee extended. Drop the lower leg over the side of the bed with gravity and support at the angle of catch or clonus. Useful for people unable to lie prone or on a small plinth. |
| Measurement considerations | Full knee extension = 0° Flexion = +ve Hyperextension = -ve |
| Starting limb position | Hip neutral, knee extended. |
| End limb position | Maximum knee flexion. Speed is V2. |
| Phase of gait cycle | Acts eccentrically in terminal stance. |
| Gait cycle observation | May contribute to knee hyperextension in stance phase, and stiff-legged gait in swing phase. |
Goniometer landmarks
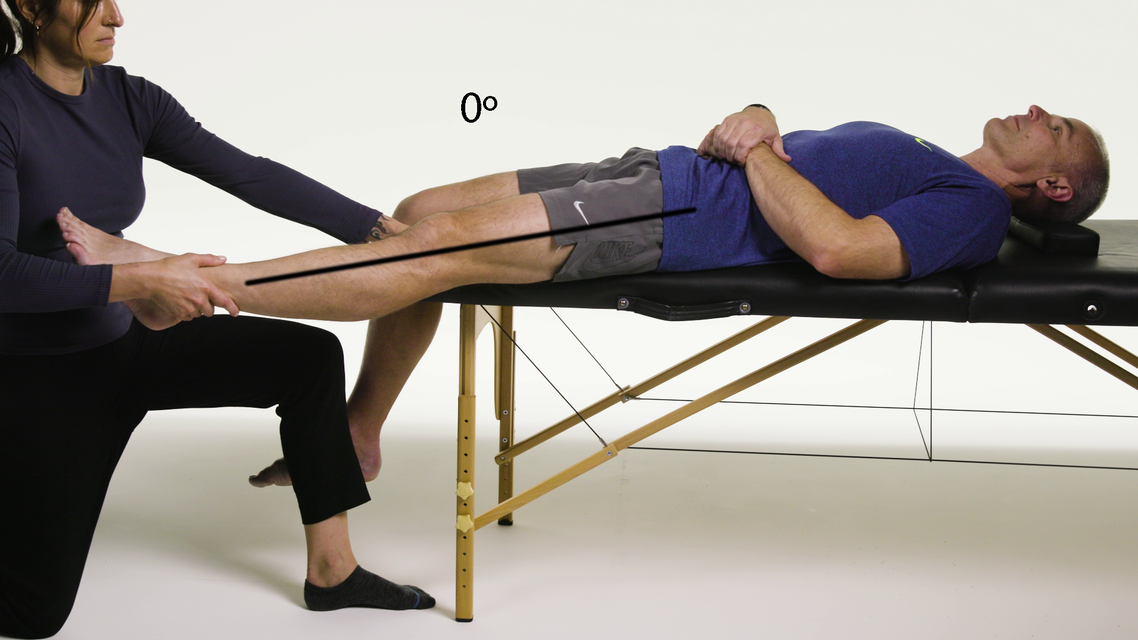
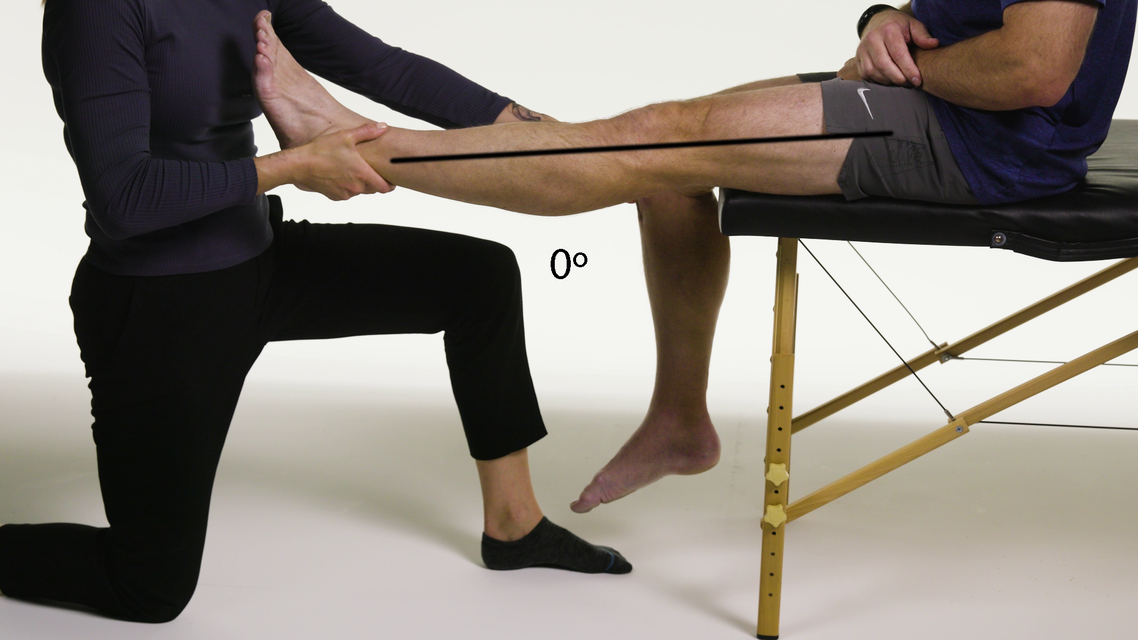
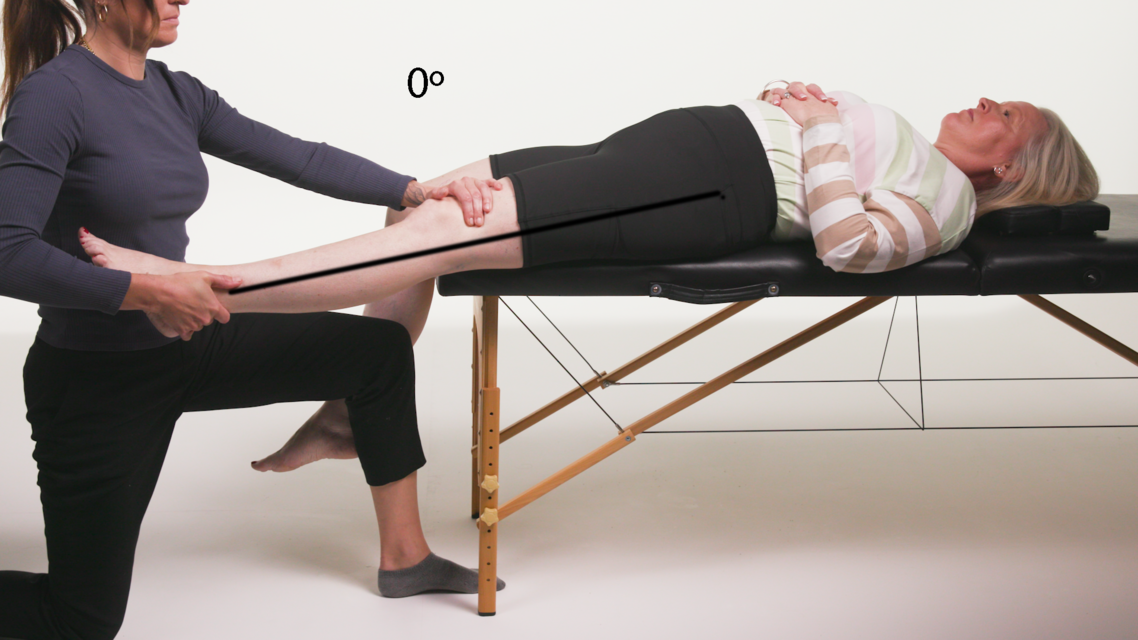
START:Control
Starting position: 0° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia

FINISH:Control
Finishing position(R2): 110° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
Control - Lateral view
START:Patient
Starting position: 0° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
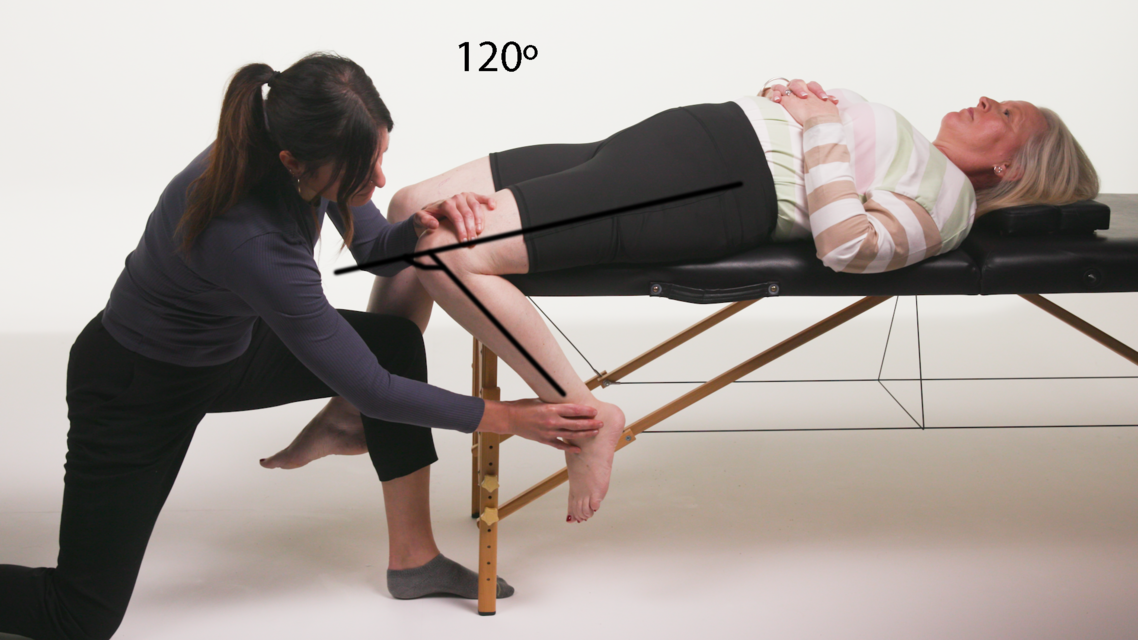
FINISH:Patient
Finishing position(R2): 120° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia

REACTION:Patient
Angle of muscle reaction (R1): 45° flexionStationary arm: femur
Axis: knee joint
Moving arm: tibia
Spasticity angle = 75°
Patient - Lateral view
Gastrocnemius
Ankle Plantarflexors
| Gastrocnemius | |
|---|---|
| Action | Plantarflexion of the ankle; flexion of the knee. |
| Origin | Medial head: above the medial femoral condyle. Lateral head: above the lateral femoral condyle. |
| Insertion | Dorsum of the calcaneus via the Achilles tendon. |
| Innervation | Tibial nerve. |
| Differential diagnosis | Differentiate from soleus with knee flexion. |
| Notes | Gastrocnemius is associated with dynamic activities, such as jumping and running. |
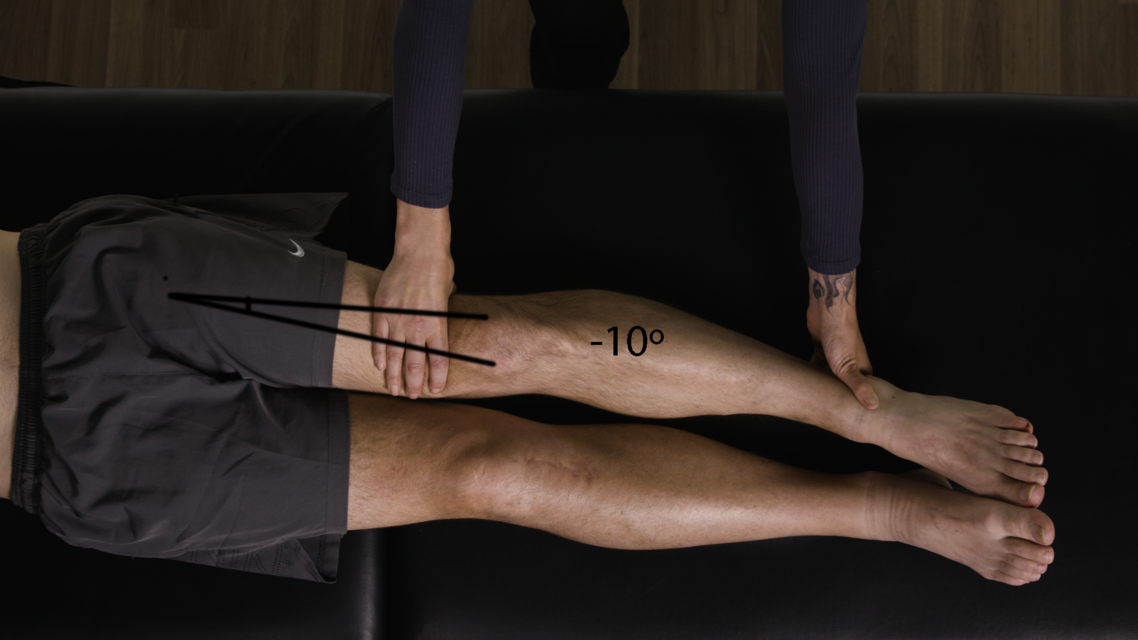
| Tardieu Testing | |
| Patient position | Supine. |
| Measurement considerations | PG = 0° PF = -ve DF = +ve |
| Starting limb position | Knee in full extension, ankle in full PF. |
| End limb position | Knee extended with maximum ankle DF. |
| Phase of gait cycle | Midstance and early swing phase. |
| Gait cycle observation | Reduced foot clearance in swing phase, potentially exhibiting drop foot with active DF (i.e. not a flaccid drop foot). |
| Other considerations | Soleus may contribute to reduced foot clearance in swing phase and knee hyperextension in stance phase. Differentiate from soleus with knee flexion. |
Goniometer landmarks
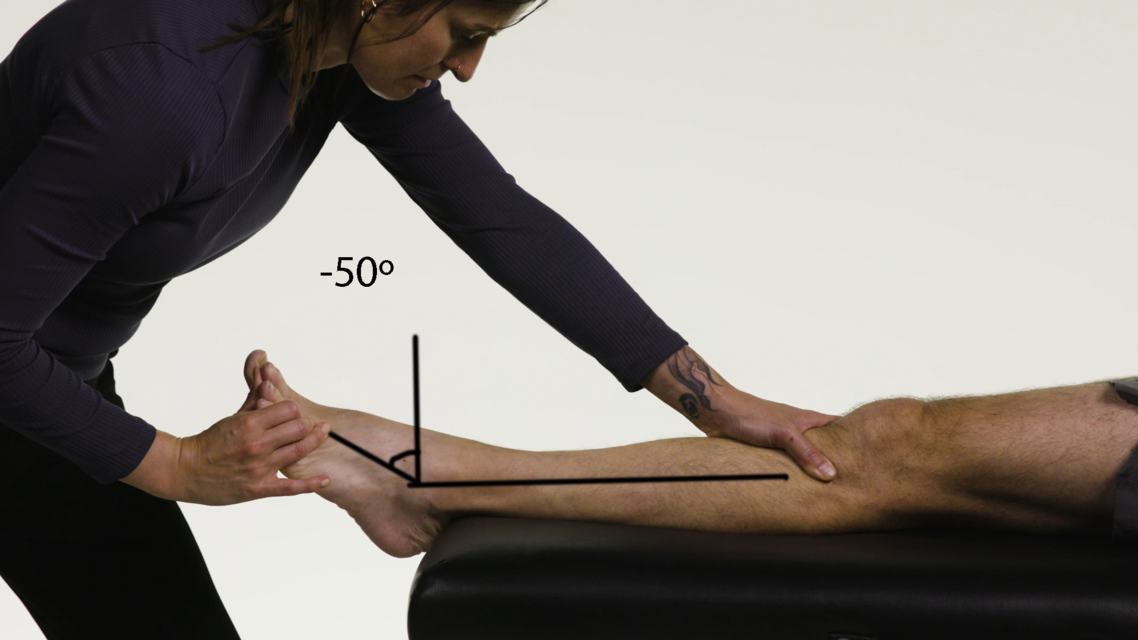
START:Control
Starting position: -50° dorsiflexionStationary arm: tibia
Axis: ankle joint
Moving arm: parallel with the sole of the foot
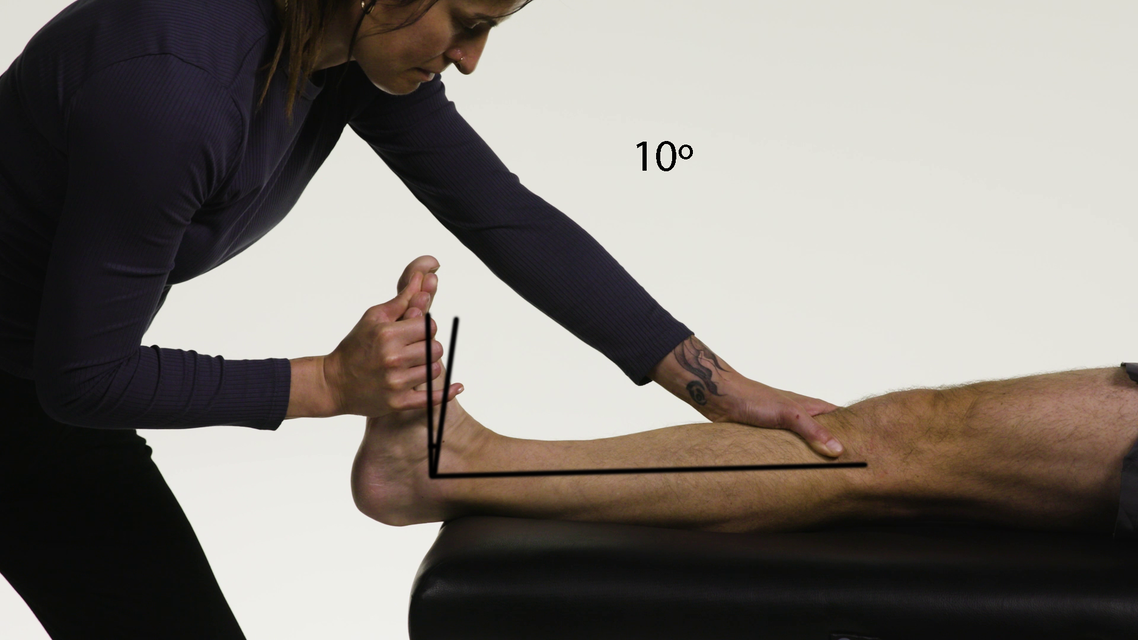
FINISH:Control
Finishing position(R2): 10° dorsiflexionStationary arm: tibia
Axis: ankle joint
Moving arm: parallel with the sole of the foot
Control - Lateral view
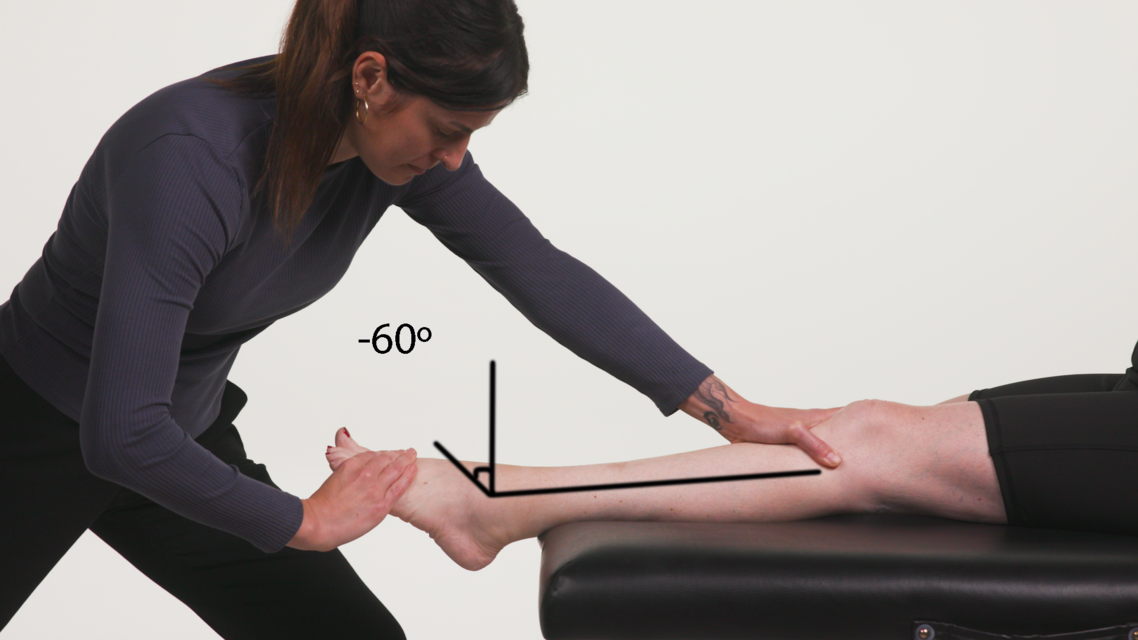
START:Patient
Starting position: -60° dorsiflexionStationary arm: tibia
Axis: ankle joint
Moving arm: parallel with the sole of the foot
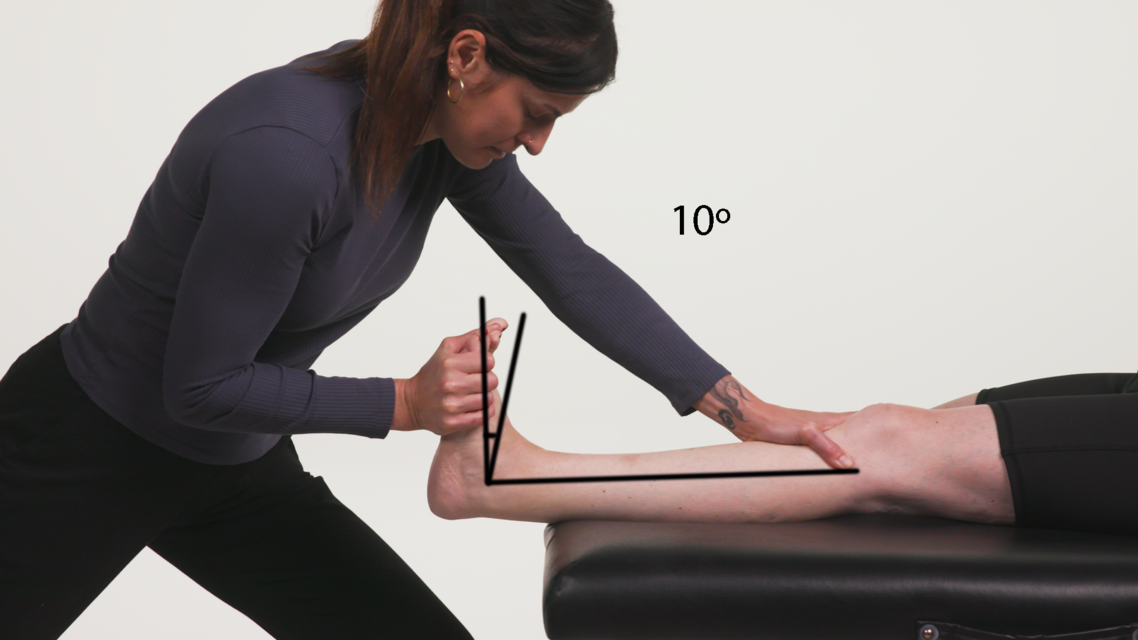
FINISH:Patient
Finishing position(R2): 10° dorsiflexionStationary arm: tibia
Axis: ankle joint
Moving arm: parallel with the sole of the foot
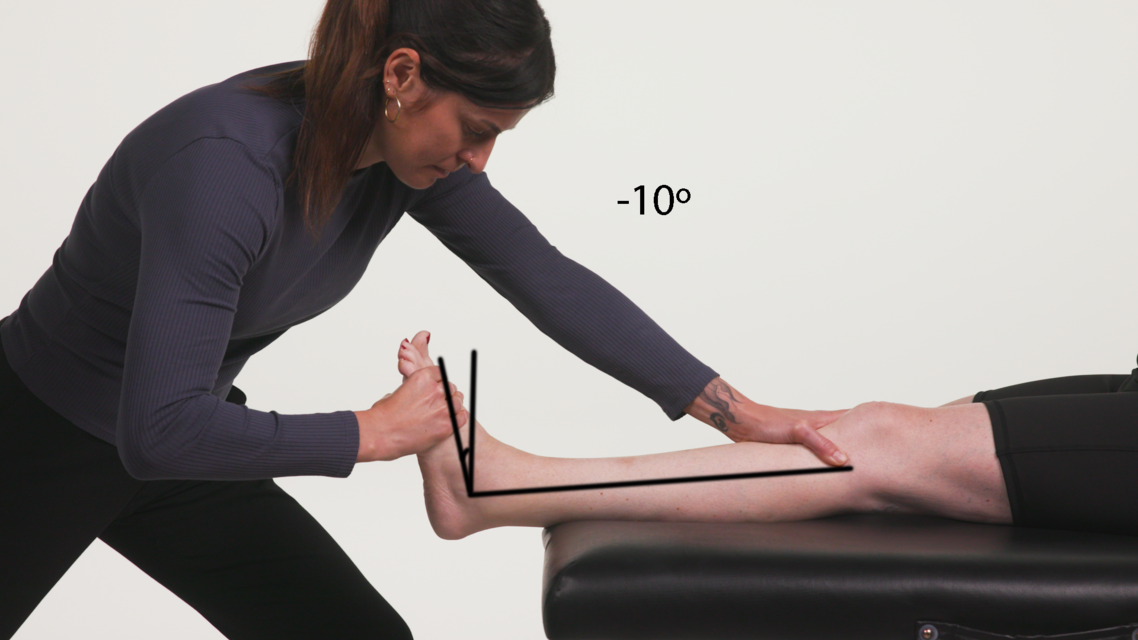
REACTION:Patient
Angle of muscle reaction (R1): -10° dorsiflexionStationary arm: tibia
Axis: ankle joint
Moving arm: parallel with the sole of the foot
Spasticity angle = 20°
Patient - Lateral view
Soleus
Ankle Plantarflexors
| Soleus | |
|---|---|
| Action | Plantarflexion of the ankle. |
| Origin | Posterior surface of the head and upper shaft of the fibula, the soleal line of the tibia. |
| Insertion | Dorsum of the calcaneus via the Achilles tendon. |
| Innervation | Tibial nerve. |
| Differential diagnosis | Differentiate from gastrocnemius with knee extension. |
| Tardieu Testing | |
| Patient position | Supine. |
| Measurement considerations | PG = 0° PF = -ve DF = +ve |
| Starting limb position | Knee flexed at 90°, ankle in full PF. |
| End limb position | Maintain knee flexed at 90° with maximum ankle DF. |
| Phase of gait cycle | Midstance and early swing phase. |
| Gait cycle observation | Hyperextension of the knee in stance phase and reduced foot clearance in swing phase, potentially exhibiting drop foot with active DF (i.e. not a flaccid drop foot). Soleus may contribute to reduced foot clearance in swing phase and knee hyperextension in stance phase. |
| Other considerations | Differentiate from gastrocnemius with knee extension. |
Goniometer landmarks
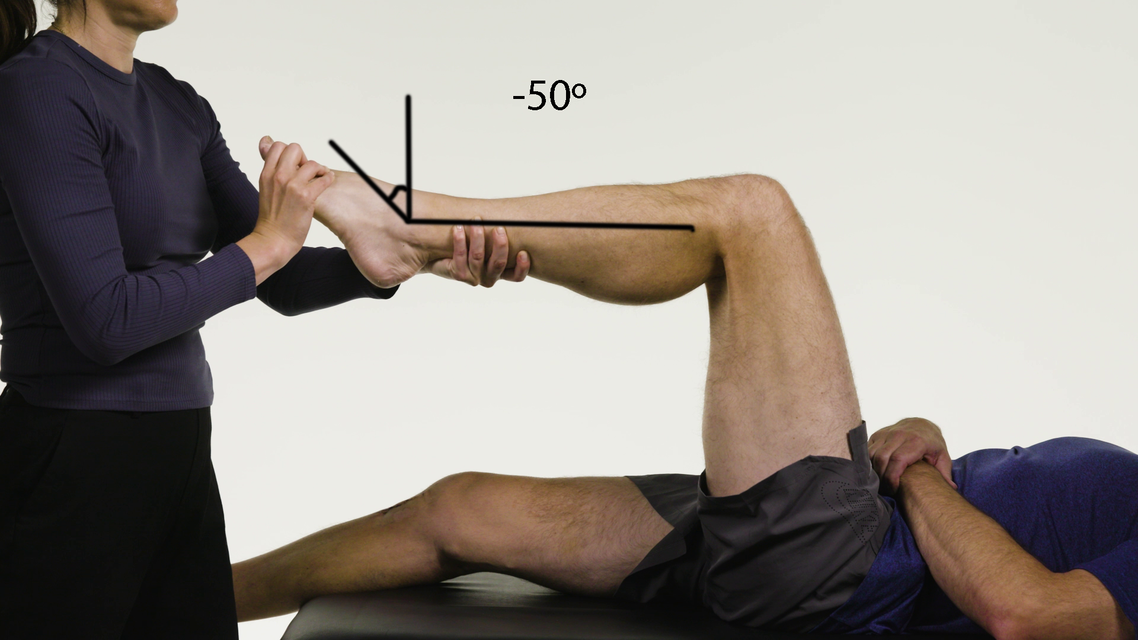
START:Control
Starting position: -50° dorsiflexionStationary arm: tibia
Axis: ankle joint
Moving arm: parallel with the sole of the foot
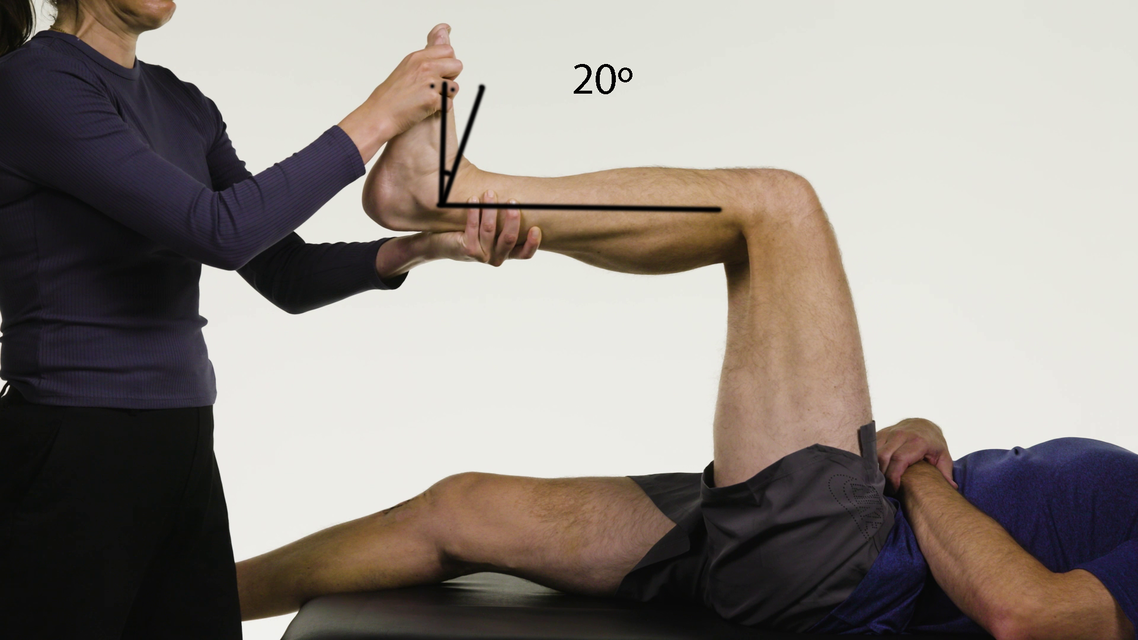
FINISH:Control
Finishing position(R2): 20° dorsiflexionStationary arm: tibia
Axis: ankle joint
Moving arm: parallel with the sole of the foot
Control - Lateral view
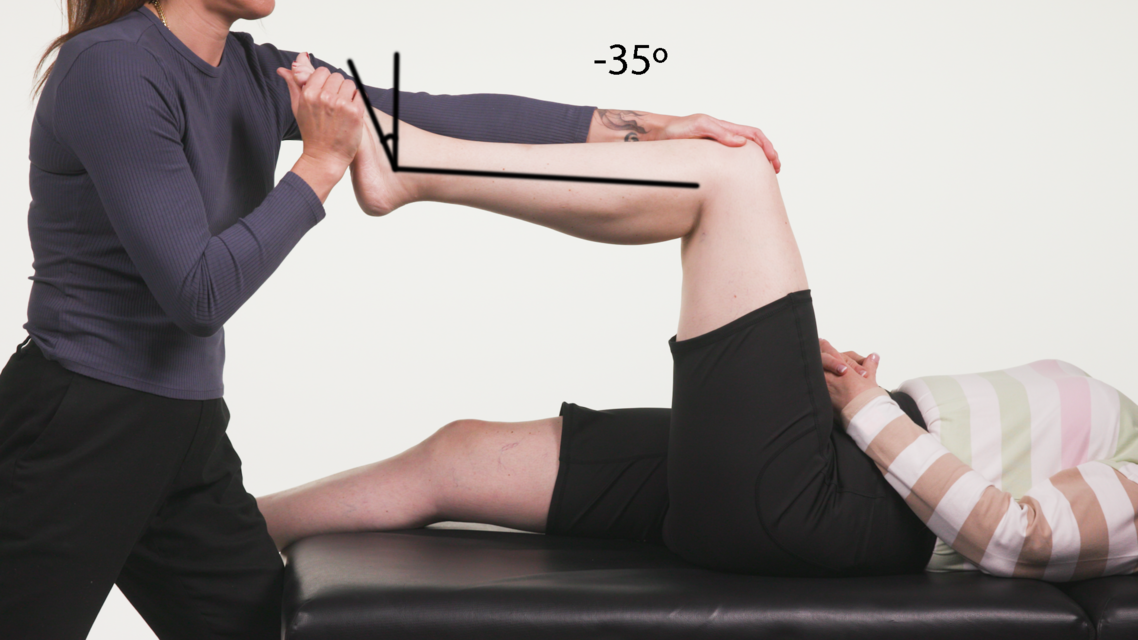
START:Patient
Starting position: -35° dorsiflexionStationary arm: tibia
Axis: ankle joint
Moving arm: parallel with the sole of the foot

FINISH:Patient
Finishing position(R2): 5° dorsiflexionStationary arm: tibia
Axis: ankle joint
Moving arm: parallel with the sole of the foot

REACTION:Patient
Angle of muscle reaction (R1): -20° dorsiflexionStationary arm: tibia
Axis: ankle joint
Moving arm: parallel with the sole of the foot
Spasticity angle = 25°
Patient - Lateral view
Tibialis Posterior
Ankle Invertor
| Tibialis Posterior | |
|---|---|
| Action | Foot inversion, assists in plantarflexion. |
| Origin | Interosseous membrane, posteromedial surface of the fibula, posterolateral surface of the tibia. |
| Insertion | Tuberosity of the navicular, cuneiform bones, cuboid, metatarsals 2 to 4. |
| Innervation | Tibial nerve. |
| Tardieu Testing | |
| Patient position | Supine. |
| Measurement considerations | Measure through the second metatarsal. Neutral ankle joint = 0° Inversion = -ve Eversion = +ve |
| Starting limb position | Ankle in full PF and inversion. |
| End limb position | Maximum ankle eversion maintaining PF at the ankle. |
| Phase of gait cycle | Stance phase. |
| Gait cycle observation | Inversion (i.e. patient is on the outer boarder of their foot) during stance. Often presents as equinovarus (inversion and plantarflexion). |
| Other considerations | Observation of equinovarus during swing phase is likely a result of tibialis anterior, whereas equinovarus during stance phase is more likely to be due to tibialis posterior. To differentiate tibialis posterior spasticity from PF spasticity, test in plantarflexion. |
Goniometer landmarks
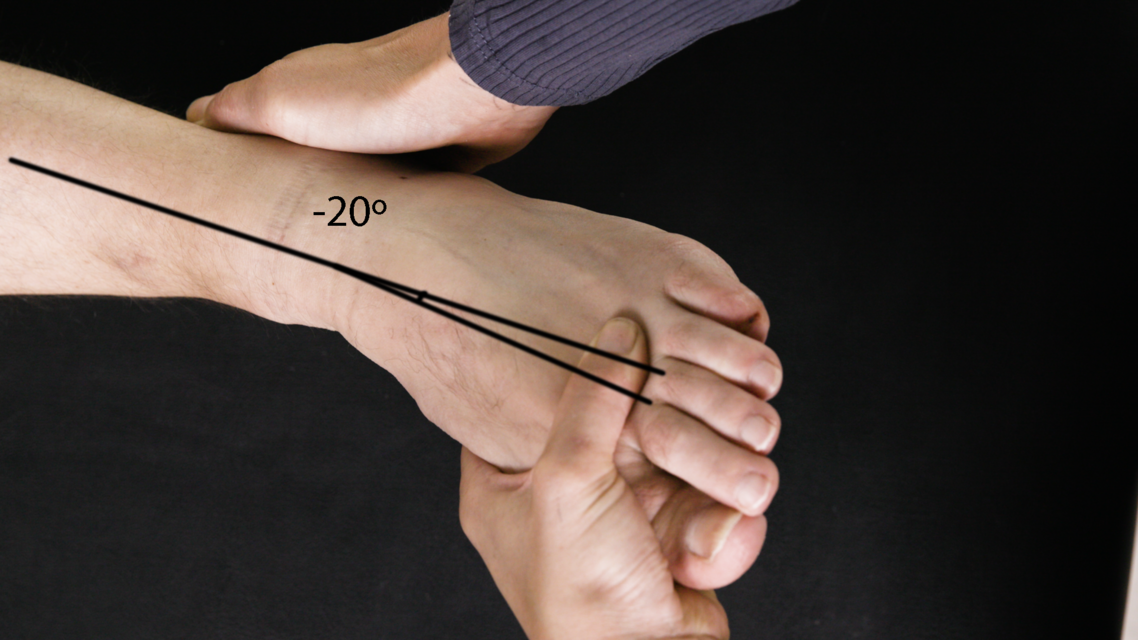
START:Control
Starting position: -20° eversionStationary arm: tibia
Axis: ankle joint
Moving arm: 2nd metatarsal

FINISH:Control
Finishing position(R2): 15° eversionStationary arm: tibia
Axis: ankle joint
Moving arm: 2nd metatarsal
Control - Aerial view

START:Patient
Starting position: -15° eversionStationary arm: tibia
Axis: ankle joint
Moving arm: 2nd metatarsal

FINISH:Patient
Finishing position(R2): 25° eversionStationary arm: tibia
Axis: ankle joint
Moving arm: 2nd metatarsal

REACTION:Patient
Angle of muscle reaction (R1): 10° eversionStationary arm: tibia
Axis: ankle joint
Moving arm: 2nd metatarsal
Spasticity angle = 15°
Patient - Aerial view
Flexor Digitorum Longus
Toe Flexors
| Flexor Digitorum Longus | |
|---|---|
| Action | Flexes the metatarsophalangeal, PIP and DIP joints of digits 2 to 5; plantarflexes the foot. |
| Origin | Posterior surface of the tibia, below the soleal line. |
| Insertion | Bases of the distal phalanges of digits 2 to 5. |
| Innervation | Tibial nerve. |
| Notes | The long toe flexors are active in the mid-stance phase of walking. The FHL and FDL assist in raising the heel from the ground. |
| Tardieu Testing | |
| Patient position | Supine. |
| Measurement considerations | Measure the DIP joint. Neutral extension = 0° Hyperextension = +ve Flexion = -ve |
| Starting limb position | Maximum knee extension with the ankle joint plantargrade, PIP joint neutral and maximum flexion of the DIP joint. |
| End limb position | Maximum knee extension with the ankle plantargrade, PIP joint neutral and maximum extension of the DIP joint. |
| Phase of gait cycle | Terminal stance. |
| Gait cycle observation | Toe clawing during mid to terminal stance. |
| Other considerations | Differentiate from short toe flexors +/- ankle DF. Callous and reddening of the top of the toes may be indicative of spasticity of the toe flexors. |
Goniometer landmarks
 2.png)
START:Control
Starting position: -65° extensionStationary arm: middle phalanx
Axis: distal interphalangeal joint
Moving arm: distal phalanx
 3.png)
FINISH:Control
Finishing position(R2): 0° extensionStationary arm: middle phalanx
Axis: distal interphalangeal joint
Moving arm: distal phalanx
Control - Lateral view
 2.png)
START:Patient
Starting position: -45° extensionStationary arm: middle phalanx
Axis: distal interphalangeal joint
Moving arm: distal phalanx
 3.png)
FINISH:Patient
Finishing position(R2): 0° extensionStationary arm: middle phalanx
Axis: distal interphalangeal joint
Moving arm: distal phalanx
 5.png)
REACTION:Patient
Angle of muscle reaction (R1): -30° extensionStationary arm: middle phalanx
Axis: distal interphalangeal joint
Moving arm: distal phalanx
Spasticity angle = 30°
Patient - Lateral view
Flexor Digitorum Brevis
Toe Flexors
| Flexor Digitorum Brevis | |
|---|---|
| Action | Flexes the metatarsophalangeal and PIP joints of digits 2 to 5. |
| Origin | Tuberosity of the calcaneus, plantar aponeurosis, intermuscular septae. |
| Insertion | Base of the middle phalanx of digits 2 to 5 after splitting to allow passage of the FDL tendons. |
| Innervation | Medial plantar nerve. |
| Notes | Flexor hallucis brevis flexes the metatarsophalangeal joint of the great toe (a task that is critical in gait). |
| Tardieu Testing | |
| Patient position | Supine. |
| Measurement considerations | Test each toe separately. Measure the PIP joint with the DIP joint in extension. Neutral = 0° Hyperextension = +ve Flexion = -ve |
| Starting limb position | Maximum knee extension with the ankle joint plantarflexed, DIP joint extension and maximum flexion of the PIP joint. |
| End limb position | Maximum knee extension with the ankle joint plantarflexed, DIP joint extension and maximum extension of the PIP joint. |
| Phase of gait cycle | Terminal stance. |
| Gait cycle observation | Toe clawing during mid to terminal stance. |
| Other considerations | Differentiate from the long toe flexors +/- ankle dorsiflexion. Callous and reddening of the top of the toes may be indicative of increased spasticity of the toe flexors. |
Goniometer landmarks
 2.png)
START:Control
Starting position: -50° extensionStationary arm: proximal phalanx
Axis: proximal interphalangeal joint
Moving arm: middle phalanx
 3.png)
FINISH:Control
Finishing position(R2): 0° extensionStationary arm: proximal phalanx
Axis: proximal interphalangeal joint
Moving arm: middle phalanx
Control - Lateral view
 2.png)
START:Patient
Starting position: -60° extensionStationary arm: proximal phalanx
Axis: proximal interphalangeal joint
Moving arm: middle phalanx
 3.png)
FINISH:Patient
Finishing position(R2): 0° extensionStationary arm: proximal phalanx
Axis: proximal interphalangeal joint
Moving arm: middle phalanx
 5.png)
REACTION:Patient
Angle of muscle reaction (R1): -15° extensionStationary arm: proximal phalanx
Axis: proximal interphalangeal joint
Moving arm: middle phalanx
Spasticity angle = 15°
Patient - Lateral view
Flexor Hallucis Longus
Toe Flexors
| Flexor Hallucis Longus | |
|---|---|
| Action | Flexes the IP joint of big toe. |
| Origin | Middle half of the posterior surface of the tibia and interosseous membrane. |
| Insertion | Bases of the distal phalanges of the great toe. |
| Innervation | Tibial nerve. |
| Notes | The long toe flexors are active in the mid-stance phase of walking. The FHL and FDL assist in raising the heel from the ground. |
| Tardieu Testing | |
| Patient position | Supine. |
| Measurement considerations | Measure the IP joint of the big toe Neutral extension = 0° Hyperextension = +ve Flexion = -ve |
| Starting limb position | Maximum knee extension with the ankle dorsiflexed, with neutral metatarsophalangeal joint and maximum flexion of the IP joint. |
| End limb position | Maximum knee extension with the ankle dorsiflexed, with neutral metatarsophalangeal joint and maximum extension of the IP joint. |
| Phase of gait cycle | Mid to terminal stance. |
| Gait cycle observation | First IP joint flexion or clawing of the big toe. |
| Other considerations | Callous and reddening of the tip of the big toe may be indicative of spasticity of the FHL. |
Goniometer landmarks
 2.png)
START:Control
Starting position: -60° extensionStationary arm: proximal phalanx
Axis: interphalangeal joint
Moving arm: distal phalanx
 3.png)
FINISH:Control
Finishing position(R2): 0° extensionStationary arm: proximal phalanx
Axis: interphalangeal joint
Moving arm: distal phalanx
Control - Lateral view
 2.png)
START:Patient
Starting position: -40° extensionStationary arm: proximal phalanx
Axis: interphalangeal joint
Moving arm: distal phalanx
 3.png)
FINISH:Patient
Finishing position(R2): 0° extensionStationary arm: proximal phalanx
Axis: interphalangeal joint
Moving arm: distal phalanx
 5.png)
REACTION:Patient
Angle of muscle reaction (R1): -15° extensionStationary arm: proximal phalanx
Axis: interphalangeal joint
Moving arm: distal phalanx
Spasticity angle = 15°
Patient - Lateral view
Appendix 1: Case Study
Patient background
Demographics
Age: 39 years old
Gender: Female
Past Medical History
- Spina Bifida diagnosed at 2 years of age
- Surgical repair of lumbar spine as child: laminectomy, detethering of spinal cord, removal of lipomas
- Developed back and neck pain in teens – laminectomy and detethering
Previous spasticity intervention
Oral medications:
- Baclofen – has trialled various doses (currently 3 x 10mg/day)
Botulinum toxin-A injections:
- Intermittently from 25 years old until present
Surgical intervention:
- Bilateral Achilles tendon release as an 8-year-old for toe walking
- Lower limbs surgeries completed when 34 years old:
- Vulpius calf lengthening Right leg
- Strayer’s calf lengthening Left leg
- Aponeurotic lengthening tibialis posterior bilaterally
- Wore AFO’s for approximately 1 year post surgery then weaned as aggravated back pain and did not like aesthetics
Assistive devices:
- Trialled different AFO’s and shoe inserts throughout childhood, adolescence and adulthood with varied effectiveness
Social history
- Lives at home with husband and two young sons (2yo and 8yo)
- Works 3 days/week in disability support (admin-based role)
- Enjoys spending time with friends and family and being fit and active
Previous level of function
- Independent mobility throughout childhood
- Was able to run as a child
- Significant mobility decline and increase in low back pain following 2nd pregnancy (required a frame and was a household ambulator for last 2 months of pregnancy)
- Has been seeing a sport physiotherapist for >10 years focussing on strengthening ankle dorsiflexors and hip extensors
- Minimal neurological physiotherapy input
Patient assessment
History of presenting complaint
Referral to spasticity clinic reporting the following primary physical concerns:- Difficulty keeping up with young children for longer distances e.g. walking to school or playing at the park
- Reduced bilateral foot clearance causing stumbles, trips and falls
- Increase in global bilateral lower limb tightness (rated as 8/10 on an average over the past 7 days)
- Increase in low back pain (rated as 5/10 when standing or sitting)
- Difficulty accessing feet and dressing lower limbs, rated as 6/10
- Requiring rail to ascend and descend stairs, currently descending backwards (carries young son up flight of stairs, safety risk to her and her son)
- Unable to wear heels (has two functions later in the year requiring heels)
- Unable to walk to coffee shop with colleagues
- Right tibial torsion and femoral anteversion causing knee varus & extension thrust in mid-stance & increased valgus in swing
- Right and left gastrocnemius, soleus and tibialis posterior spasticity & hypertonicity contributing to reduced dorsiflexion in swing & increased inversion at push off, as well as knee hyperextension & plantarflexion coupling in stance
- Right and left co-contraction of rectus femoris & medial hamstring bilaterally causing increased knee flexion at initial contact & reduced knee extension at terminal swing
- Bilateral hip extensor weakness, abdominal weakness & lumbar spine hyper-lordosis contributing to increased anterior pelvic tilt & posterior trunk lean throughout gait
- Bilateral hip abductor & pelvic weakness contributing to right Trendelenburg & pelvic retraction throughout gait
Initial Functional Assessment
| Pre- Injection Mobility | |
|---|---|
| Transfers | Independent, no aids (FIM 7) |
| Gait | Independent indoors and outdoors, no aid (FIM 7) |
| Stairs |
Independent, with rail, reciprocal pattern (FIM 6)
Note: descends stairs backwards to assist with knee control |
| 10 metre walk test | Self-selected: 8.8s, 0.9m/s
Fast: 6.1s, 1.6m/s Note: walking speed was not a reported concern compared to walking quality especially over longer distances |
| 6-minute walk test | 480m, 1.3m/sec
4 x catch on left and 6 x catches on right |
| Walking endurance | Dependent on speed, terrain, crowds
10 minutes before increased falls risk and catching |
| Falls | Variable - can be several per day or months without
5 falls over prior month reported |
| Running | Unable |
Initial Physical Assessment
Hip assessment
| Left | Right | ||
|---|---|---|---|
| Flexors | R2 (PROM extension) | 20° | 20° |
| R1 (muscle reaction) | 0° | 20° | |
| Tardieu score | 2 | 1 | |
| Strength | 4/5 | 4/5 | |
| Extensors | PROM (flexion, knee @ 90°) | 125° | 125° |
| Strength | 3/5 | 3/5 | |
| Adductors | R2 (PROM abduction) | 35 | 35 |
| R1 (muscle reaction) | 35 | 35 | |
| Tardieu Score | 1 | 1 | |
| Strength | 4/5 | 4/5 | |
| Abductors | Strength | 3/5 | 3/5 |
Knee assessment
| Left | Right | ||
|---|---|---|---|
| Flexors | R2 @ 90° HF (PROM extension) | -35° | -10° |
| R1 @ 90° HF (muscle reaction) | -75° | -50° | |
| Tardieu score @ 90° HF | 2 | 2 | |
| R2 @ 30° HF (PROM extension) | 0 | 0° | |
| R1 @ 30° HF (muscle reaction) | -40° | -20° | |
| Tardieu score @ 30° HF | 2 | 2 | |
| Strength | 2/5 | 3/5 | |
| Extensors | R2, RF (PROM flexion) | 135° | 135° |
| R1, RF (muscle reaction) | 50° | 100° | |
| Tardieu score, RF | 2 | 2 | |
| R2, vastii (PROM flexion) | 115° | 115° | |
| R1, vastii (muscle reaction) | 65° | 90° | |
| Tardieu score, vastii | 2 | 2 | |
| Strength | 4/5 | 4/5 | |
Knee flexors
Knee extensors
Ankle assessment
| Left | Right | ||
|---|---|---|---|
| Plantarflexors | R2, gastroc (PROM DF) | 25° | 25° |
| R1, gastroc (muscle reaction) | -5° | 10° | |
| Tardieu score, gastroc | 4 | 2 | |
| R2, soleus (PROM DF) | 5° | 15° | |
| R1, soleus (muscle reaction) | -15° | 0° | |
| Tardieu score, soleus | 4 | 2 | |
| Strength | 4/5 | 4/5 | |
| Dorsiflexors | PROM (PF) | 40° | 40° |
| Strength | 3/5 | 4/5 | |
| Invertors | R2, tib post (PROM eversion) | 40° | 40° |
| R1, tib post (muscle reaction) | 15° | 40° | |
| Tardieu score, tib post | 3 | 1 | |
| Strength | 4/5 | 4/5 | |
| Evertors | PROM (inversion) | 45° | 45° |
| Strength | 3/5 | 4/5 | |
Ankle PF’s
Ankle invertors
Goal attainment scale
Patient goal #1: I want to walk up and down a flight of stairs independently
SMART goal #1: To be able to ascend/descend 14 stairs independently, with 1 x rail, forward facing and using a reciprocal pattern in 8 weeks
| +2 | Much better than expected | Ascend/descend 14 stairs independently, reciprocal pattern with no rail, forward facing in 8/52 |
| +1 | More than expected | Ascend 14 stairs with no rail, and descend with 1 x rail, independently, forward facing, reciprocal pattern in 8/52 |
| 0 | Likely (predicted) outcome | Ascend/descend 14 stairs independently with 1 x rail, forward facing and reciprocal pattern in 8/52 |
| -1 | Less than expected outcome | Requires either 2 x rails or a non-reciprocal pattern to ascend/descend 14 stairs independently, forward facing in 8/52 |
| -2 | Much less than expected outcome | Unable to ascend/descend 14 stairs independently, forward facing, in 8/52 |
Patient goal #2: I want to stumble less when I walk
SMART goal #2: To be able to reduce frequency of toe catching during a 6-minute walk test from 10 to ≤5 in 8 weeks
| +2 | Much better than expected | 0 episodes of toe catching during a 6mwt in 8/52 |
| +1 | More than expected | 1-2 episodes of toe catching during a 6mwt in 8/52 |
| 0 | Likely (predicted) outcome | 3-5 episodes of toe catching during a 6mwt in 8/52 |
| -1 | Less than expected outcome | 5-8 episodes of toe catching during a 6mwt in 8/52 |
| -2 | Much less than expected outcome | >8 episodes of toe catching during a 6mwt in 8/52 |
Patient goal #3: I want to look less disabled when I walk
SMART goal #3: Improve self-rated quality of walking from 4/10 to ≥6/10 in 8 weeks
**Note: quality rated as an average of all walking over the previous 7 days| +2 | Much better than expected | Self-rated walking quality: 9-10/10 in 8/52 |
| +1 | More than expected | Self-rated walking quality: 7-8/10 in 8/52 |
| 0 | Likely (predicted) outcome | Self-rated walking quality: 5-6/10 in 8/52 |
| -1 | Less than expected outcome | Self-rated walking quality: 3-4/10 in 8/52 |
| -2 | Much less than expected outcome | Self-rated walking quality: 0-2/10 in 8/52 |
Patient intervention
Multidisciplinary team decision
- Botulinum toxin-A injections to left lower limb as per table below
| Muscle, Dosage and Technique | Rationale & considerations |
|---|---|
|
Gastrocnemius
100u (50u each head) U/S |
|
|
Soleus
100u U/S |
|
|
Tibialis posterior
75u U/S |
|
|
Rectus femoris
100u <(50u, 2 x sites) U/S |
|
- Twice weekly physiotherapy and once weekly exercise physiology
- Daily home exercise and walk program
- Review in spasticity clinic in 8 weeks
- Re-assess goal attainment
- Re-assess bilateral spasticity, strength and function
- Further consideration of left hamstring and right calf botulinum toxin-A injection
Physiotherapy program
- Comprehensive exercise program to include:
- Strengthening and ROM of ankle plantarflexors, dorsiflexors and evertors
- Strengthening of knee flexors and extensors predominantly eccentrically
- Hip and pelvic complex dissociation and activation
- Ongoing trunk mobility and stability
- Gait re-training
- Cardiovascular fitness
- Re-explore assistive devices to assist with foot clearance and maximise safety including AFO’s and ASO’s
- Trial toe spreaders
- Trial community mobility devices to enhance participation with family and help fatigue management
Patient review (8-weeks post Botulinum Toxin-A injection)
Functional Review
| Pre- Injection Mobility | Post- Injection Mobility | |
|---|---|---|
| Transfers | Independent, no aids (FIM 7) | Independent, no aids (FIM 7) |
| Gait | Independent indoors and outdoors, no aid (FIM 7) | Independent indoors and outdoors, no aid (FIM 7) |
| Stairs | Independent, with rail, reciprocal pattern (FIM 6) | Independent, no rail, reciprocal pattern (FIM 7) |
| 10 metre walk test |
Self-selected: 8.8s, 0.9m/s
Fast: 6.1s, 1.6m/s |
Self-selected: 7.5s, 1.3m/s
Fast: 5.5s, 1.8m/s |
| 6-minute walk test |
480m, 1.3m/sec
4 x catch on L and 6 x catches on R |
544m, 1.5m/sec
1 x catch on L and 2 x catches on R |
| Walking endurance | 10 minutes before ↑ falls risk and catching | 15 minutes before ↑ falls risk and catching |
| Falls | 5 falls over prior month | 2 falls over prior month |
| Running | Unable | Unable |
Goal Review
| Goal | Pre-injection | Post-injection | GAS rating |
|---|---|---|---|
| Stairs | Independent, with rail, reciprocal pattern, descending backwards | Independent, no rail, reciprocal pattern, forward facing | +2 |
| Toe catching | 10 catches during 6mwt | 3 catches during 6mwt | +1 |
| Walking quality | Self-rated quality of walking: 4/10 | self-rated quality of walking: 6/10 | 0 |
References
- Ansari, N. N., Naghdi, S., Arab, T. K., & Jalaie, S. (2008). The interrater and intrarater reliability of the Modified Ashworth Scale in the assessment of muscle spasticity: limb and muscle group effect. Neuro Rehabil, 23(3), 231-237.
- Ansari, N. N., Naghdi, S., Arab, T. K., & Jalaie, S. (2008). The interrater and intrarater reliability of the Modified Ashworth Scale in the assessment of muscle spasticity: limb and muscle group effect. Neuro Rehabil, 23(3), 231-237.
- Ansari, N. N., Naghdi, S., Moammeri, H., & Jalaie, S. (2006). Ashworth Scales are unreliable for the assessment of muscle spasticity. Physiother Theory Pract, 22(3), 119-125.
- Ansari, N. N., Naghdi, S., Younesian, P., & Shayeghan, M. (2008). Inter- and intrarater reliability of the Modified Modified Ashworth Scale in patients with knee extensor poststroke spasticity. Physiother Theory Pract, 24(3), 205-213. doi: 10.1080/09593980701523802
- Ashford, S., & Turner-Stokes, L. (2006). Goal attainment for spasticity management using botulinum toxin Physiother Res Int, 11(1), 24-34. doi:10.1002/pri.36
- Ashford, S., & Turner-Stokes, L. (2018). Spasticity in adults: Management using botulinum toxin: National guidelines. London: Royal College of Physicians of London.
- Ashford, S., & Turner-Stokes, L. (2013). Systematic review of upper-limb function measurement methods in botulinum toxin intervention for focal spasticity. Physiother Res Int, 18(3), 178-189.
- Ashworth B. (1964). Preliminary trial of carisprodal in multiple sclerosis. Practitioner, 192:54-542.
- Boyd, R. N., & Graham, K. H. (1999). Objective measurement of clinical findings in the use of botulinum toxin type A for the management of children with cerebral palsy. Eur J of Neurol 6(S4), S23-S35.
- Brashear, A., & Elovic, E. (2010). Spasticity: Diagnosis and management. New York: Demos Medical Publishing.
- Deloitte Access Economics. (2013). The economic impact of stroke in Australia. Retrieved from http:// strokefoundation.com.au/site/media/Final-Deloitte- Stroke-Report-14-Mar-13.pdf
- Demetrios, M., Gorelik, A., Louie, J., Brand, C., Baguley, I. J., & Khan, F. (2014). Outcomes of ambulatory rehabilitation programmes following botulinum toxin for spasticity in adults with stroke. J of Rehabil Med, 46(8), 730-737 738p. doi:10.2340/16501977-1842
- Esquenazi, A., Novak, I., Sheean, G., Singer, B. J., & Ward, A. B. (2010). International consensus statement for the use of botulinum toxin treatment in adults and children with neurological impairments: Introduction. Eur J of Neurol, 17(S2), 1-8.
- Fleuren JF, Voerman GE, Erren-Wolters CV, Snoek GJ, Rietman JS, Hermens HJ et al. (2010). Stop using the Ashworth Scale for the assessment of spasticity. J Neurol Neurosurg Psychiatry, 81,46–52.
- Gracies, J. M., Elovic, E., McGuire, J., & Simpson, D. (1997). Traditional pharmacological treatments for spasticity part I: Local treatments. Muscle Nerve, 20(S6), 61-91.
- Gracies, J. M., Nance, P., Elovic, E., McGuire, J., & Simpson, D. M. (1997). Traditional pharmacological treatments for spasticity part II: General and regional treatments. Muscle Nerve, 20(S6), 92-120.
- Gracies J-M, Marosszeky J, Renton R, Sandaman J, Gandevia S, Burke D. (2000). Short term effects of dynamic lycra splints on upper limb in hemiplegia patients. Arch Phys Med Rehabil, 81:1547-1555.
- Gracies J-M, Burke K, Clegg NJ, Browne R, Rushing C, Fehlings D, Matthews D, Tilton A, Delgado MR. (2010) Reliability of the Tardieu Scale for assessing spasticity in children with cerebral palsy. Arch Phys Med Rehabil. 91(3),:421-428. doi: 10.1016/j.apmr.2009.11.017
- Haugh A, Pandyan A, Johnson G. (2006). A systematic review of the Tardieu Scale for the measurement of spasticity. Disabil Rehabil.28(15),899-907.
- Held JP, Pierrot-Deseilligny E.(1969). Reeducation Motrice des Affections Neurologiques, Paris France: JB Bailiere et Fils, 31–42
- Ivanhoe, C. B., & Reistetter, T. A. (2004). Spasticity: The misunderstood part of the upper motor neuron syndrome. Am J of Phys Med Rehab, 83(10), S3-S9. doi:10.1097/01.phm.0000141125.28611.3e
- Keenan, M., Haider, T., & Stone, L. (1990). Dynamic electromyography to assess elbow spasticity. J Hand Surg,15(4), 607-614.
- Kiresuk, T. J., & Sherman, M. R. E. (1968). Goal attainment scaling: A general method for evaluating comprehensive community mental health programs. Community Ment Health J, 4(6), 443-453.
- Lance, J. W. (1980). The control of muscle tone, reflexes, and movement: Robert Wartenberg lecture. Neurology, 30(12), 1303-1313.
- Moore E, Williams G, Olver J, Bryant A, Banky M. (2015). The effectiveness of therapy on outcome following BoNT-A injection for focal spasticity in adults with neurological conditions - systematic review. Brain Injury, 29(6), 676-687.
- Mehrholz J, Wagner K, Meissner D, Grundmann K, Zange C, Koch R et al. (2005). Reliability of the Modified Tardieu Scale and the Modified Ashworth Scale in adult patients with severe brain injury: a comparison study. Clin Rehabil, 19, 751–759.
- Olver, J., Esquenazi, A., Fung, V. S. C., Singer, B. J., & Ward, A. B. (2010). Botulinum toxin assessment, intervention and aftercare for lower limb disorders of movement and muscle tone in adults: International consensus statement. Eur J Neurol, 17(S2), 57-73.
- Pandyan, A., Gregoric, M., Barnes, M., Wood, D., Wijck, F., Burridge, J., Hermens, H., Johnson, A. (2005). Spasticity: Clinical perceptions, neurological realities and meaningful measurement. Disabil Rehabil, 27(1-2), 2-6. doi:10.1080/09638280400014576
- Pandyan, A. D., Vuadens, P., van Wijck, F. M. J., Stark, S., Johnson, G. R., & Barnes, M. P. (2002). Are we underestimating the clinical efficacy of botulinum toxin (type A)? Quantifying changes in spasticity, strength and upper limb function after injections of Botox® to the elbow flexors in a unilateral stroke population. Clin Rehabil, 16(6), 654-660.
- Pandyan, A. D., Johnson, G. R., Price, C. I., Curless, R. H., Barnes, M. P., & Rodgers, H. (1999). A review of the properties and limitations of the Ashworth and modified Ashworth Scales as measures of spasticity. Clin Rehabil, 13(5), 373-383.
- Patrick, E., & Ada, L. (2006). The Tardieu Scale differentiates contracture from spasticity whereas the Ashworth Scale is confounded by it. Clin Rehabil, 20(2), 173-181. doi: 10.1191/0269215506cr922oa
- Sanger TD, Delgado MR, Gaebler-Spira D, Hallett M, Mink JW. (2003). Task Force on childhood motor disorders, classification and definition of disorders causing hypertonia in childhood. Pediatrics,111,: e89–e97.
- Sheean, G., Lannin, N. A., Turner-Stokes, L., Rawicki, B., & Snow, B. J. (2010). Botulinum toxin assessment, intervention and after-care for upper limb hypertonicity in adults: International consensus statement. Eur J Neurol, 17(S2), 74-93.
- Singh, P., Joshua, A. M., Ganeshan, S., & Suresh, S. (2011). Intra-rater reliability of the modified Tardieu scale to quantify spasticity in elbow flexors and ankle plantar flexors in adult stroke subjects. Ann Indian Acad Neurol, 14(1), 23-26.
- Tardieu G, Rondont O, Mensch J, Dalloz J-C, Monfraix C, Tabary J-C. (1957). Responses electromyographiques a l’etirement musculaire chez l’homme normal. Rev Neurol, 97, 60-61.
- Tardieu G, Shentoub S, Delarue R. (1954). A la recherche d’une technique de measure de la spasticite. Rev Neurol, 91(2), 143-144.
- Turner-Stokes, L. (2009). Goal attainment scaling (GAS) in rehabilitation: A practical guide. Clin Rehabil, 23(4), 362-370. doi:10.1177/0269215508101742
- Urban, P. P., Wolf, T., Uebele, M., Marx, J. J., Vogt, T., Stoeter, P., Bauermann, T., Weibrich, C., Vucurevic, G.D., Schneider, A., Wissel, J. (2010). Occurence and clinical predictors of spasticity after ischemic stroke. Stroke, 41(9), 2016-2020. doi:10.1161/strokeaha.110.581991
- Williams, G., Olver, J., De Graaff, S., & Singer, B.J. (2012). The use of botulinum toxin type A in the management of adult-onset focal spasticity: A survey of Australian allied health professionals. Aust Occup Ther J, 59(4), 257-264. doi:10.1111/j.1440-1630.2012.01027.
- Yelnik, A. P., Simon, O., Parratte, B., & Gracies, J.M. (2010). How to clinically assess and treat muscle overactivity in spastic paresis. J Rehabil Med, 42(9), 801-807. doi:10.2340/16501977-0613
- Yelnik, A., Albert, T., Bonan, I., & Laffont, I. (1999). A clinical guide to assess the role of lower limb extensor overactivity in hemiplegic gait disorders. Stroke, 30(3), 580-585.
Feedback
We are interested to know your feedback and suggestions for further development of this App, please contact us at physioresearch@epworth.org.au